Tepper Stewart J, Diamond Merle L, Hirman Joe, Asher Divya, Fiore Damian, Cady Roger
New England Institute for Neurology and Headache, Stamford, CT, USA.
Diamond Headache Clinic, Chicago, IL, USA.
J Neurol. 2024 Dec 12;272(1):4. doi: 10.1007/s00415-024-12809-z.
Longer periods between headache episodes (interictal periods) may provide greater time for the nervous system to reset from a previous episode, potentially improving disease status and health-related quality of life. This post hoc analysis evaluated this hypothesis by associating patients' longest interictal periods with improvements in patient-reported outcomes.
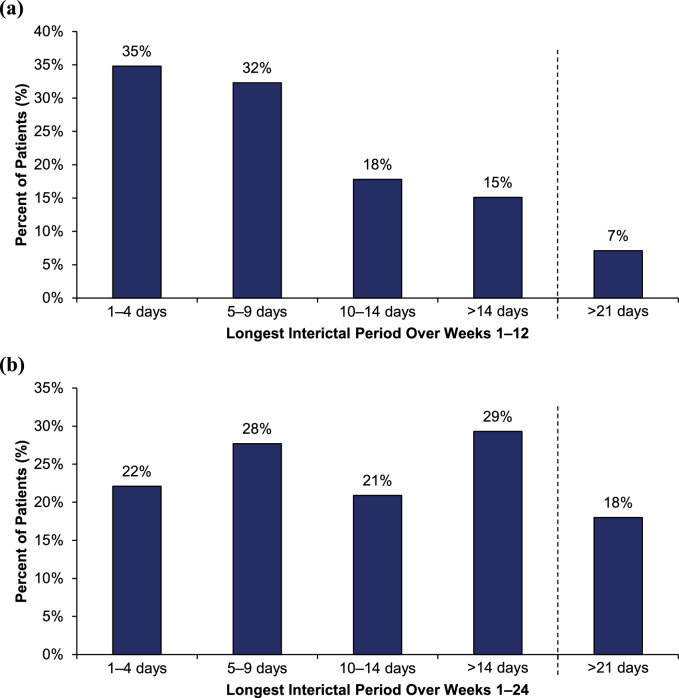
PROMISE-2 (NCT02974153) was a double-blind, placebo-controlled study evaluating eptinezumab for preventive treatment of chronic migraine (N = 1072). Daily electronic diary data from Weeks 1-12 and Weeks 1-24 were used to identify interictal periods, defined as days between headache episodes. For each patient, the longest interictal period within these intervals was identified and categorized (1-4, 5-9, 10-14, > 14, and > 21 days). For each category, the following patient-reported outcomes were assessed: 6-item Headache Impact Test (HIT-6), Patient Global Impression of Change (PGIC), and patient-identified most bothersome symptom (PI-MBS).
Excluding interictal periods with > 10% missing data (resulting in 1010 patients with sufficient data), the mean (SD) of longest interictal periods over Weeks 1-12 was 9.4 (11.0) days. A ≥6-point HIT-6 reduction was observed in 78% (56/72) vs 26% (91/351) of patients with a > 21-day vs 1-4-day longest interictal period, respectively; much or very much improvement per PGIC was reported in 90% (65/72) vs 25% (87/348), respectively, and per PI-MBS was reported in 88% (63/72) vs 26% (92/348), respectively. Similar results were observed for Weeks 1-24.
Longer interictal periods were associated with more patients indicating positive changes in headache-related life impact, disease status, and symptomology.
ClinicalTrials.gov (identifier: NCT02974153; registered: 2016-11-23).
头痛发作间期延长可能为神经系统从前一次发作中恢复提供更多时间,从而可能改善疾病状态和与健康相关的生活质量。这项事后分析通过将患者最长的发作间期与患者报告的结局改善情况相关联来评估这一假设。
PROMISE-2(NCT02974153)是一项双盲、安慰剂对照研究,评估依替奈单抗预防慢性偏头痛的效果(N = 1072)。使用第1 - 12周和第1 - 24周的每日电子日记数据来确定发作间期,发作间期定义为头痛发作之间的天数。对于每位患者,确定这些时间段内最长的发作间期并进行分类(1 - 4天、5 - 9天、10 - 14天、> 14天和> 21天)。对于每个类别,评估以下患者报告的结局:6项头痛影响测试(HIT - 6)、患者总体变化印象(PGIC)以及患者确定的最困扰症状(PI - MBS)。
排除缺失数据> 10%的发作间期(最终有1010例患者数据充足),第1 - 12周最长发作间期的均值(标准差)为9.4(11.0)天。最长发作间期> 21天的患者中,78%(56 / 72)的患者HIT - 6降低≥6分,而最长发作间期为1 - 4天的患者中这一比例为26%(91 / 351);分别有90%(65 / 72)和25%(87 / 348)的患者报告PGIC有很大或非常大的改善,分别有88%(63 / 72)和26%(92 / 348)的患者报告PI - MBS有改善。第1 - 24周观察到类似结果。
发作间期越长,表明头痛相关生活影响、疾病状态和症状学有积极变化的患者越多。
ClinicalTrials.gov(标识符:NCT02974153;注册时间:2016年11月23日)。