Bond M J G, Mijnals C, Bolhuis K, van Amerongen M J, Engelbrecht M R W, Hermans J J, van Lienden K P, May A M, Swijnenburg R-J, Punt C J A
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Department of Pathology, OLVG, Amsterdam, The Netherlands.
ESMO Open. 2024 Dec;9(12):104075. doi: 10.1016/j.esmoop.2024.104075. Epub 2024 Dec 11.
RECIST may not be optimal for assessing treatment response with current systemic regimens. We evaluated RECIST, morphologic, and pathologically documented response (pathological response) in patients with initially unresectable colorectal cancer liver-only metastases (CRLM).
Four hundred and eighty-nine patients from the phase III CAIRO5 trial were included who were treated with FOLFOX/FOLFIRI/FOLFOXIRI and bevacizumab or panitumumab. The association of the different response tools with overall survival (OS) was evaluated for all patients, and with early recurrence (<6 months) for patients after complete local treatment.
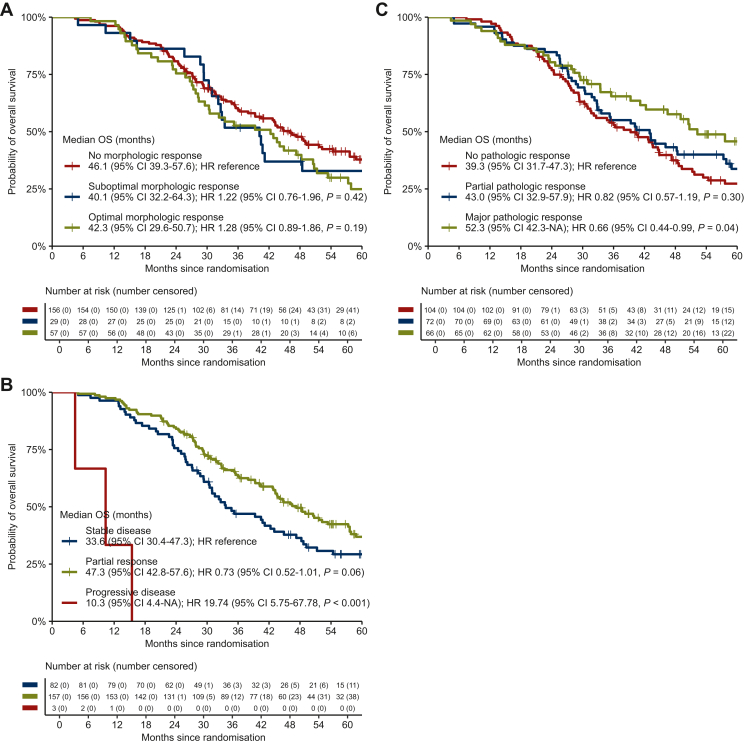
In the overall population, suboptimal [hazard ratio (HR) 1.10, 95% confidence interval (CI) 0.83-1.47] and optimal (HR 0.95, 95% CI 0.74-1.22) morphologic response were not associated with OS compared with no response. RECIST partial response (HR 0.61, 95% CI 0.49-0.76) and progressive disease (HR 5.77, 95% CI 3.97-8.39) were associated with OS compared with stable disease. In 242 patients who underwent local treatment, suboptimal (HR 1.22, 95% CI 0.76-1.96) and optimal (HR 1.28, 95% CI 0.89-1.86) morphologic response were not associated with OS compared with no response. RECIST partial response was not significantly associated with OS (HR 0.73, 95% CI 0.52-1.01), whereas progressive disease was (HR 19.74, 95% CI 5.75-67.78), compared with stable disease. While major pathological response (HR 0.66, 95% CI 0.44-0.99) was associated with OS, partial pathological response (HR 0.82, 95% CI 0.57-1.19) was not, compared with no pathological response. Pathological response, but not morphologic response and RECIST, was significantly associated with early recurrence (P < 0.001) which occurred in 13/58 (22%) patients with major response, 29/61 (48%) patients with partial response, and 51/88 (58%) patients with no response.
Our results show that RECIST but not morphologic response was prognostic for OS. In patients eligible for local treatment, neither RECIST nor morphologic response were associated with early recurrence. Pathological response was associated with early recurrence but is only available post-operatively. Hence, novel preoperative parameters are warranted to predict early recurrence and prevent potentially futile liver surgery.
实体瘤疗效评价标准(RECIST)可能并非评估当前全身治疗方案疗效的最佳方法。我们评估了最初无法切除的仅发生肝转移的结直肠癌(CRLM)患者的RECIST、形态学及病理记录的反应(病理反应)。
纳入了III期CAIRO5试验中的489例患者,这些患者接受了氟尿嘧啶/亚叶酸钙/奥沙利铂(FOLFOX)/氟尿嘧啶/亚叶酸钙/伊立替康(FOLFIRI)/氟尿嘧啶/亚叶酸钙/奥沙利铂/伊立替康(FOLFOXIRI)联合贝伐单抗或帕尼单抗治疗。评估了所有患者不同反应评估工具与总生存期(OS)的相关性,以及局部治疗后患者与早期复发(<6个月)的相关性。
在总体人群中,与无反应相比,次优形态学反应(风险比[HR]1.10,95%置信区间[CI]0.83 - 1.47)和优形态学反应(HR 0.95,95% CI 0.74 - 1.22)与OS无关。与疾病稳定相比,RECIST部分缓解(HR 0.61,95% CI 0.49 - 0.76)和疾病进展(HR 5.77,95% CI 3.97 - 8.39)与OS相关。在242例接受局部治疗的患者中,与无反应相比,次优形态学反应(HR 1.22,95% CI 0.76 - 1.96)和优形态学反应(HR 1.28,95% CI 0.89 - 1.86)与OS无关。与疾病稳定相比,RECIST部分缓解与OS无显著相关性(HR 0.73,95% CI 0.52 - 1.01),而疾病进展与OS相关(HR 19.74,95% CI 5.75 - 67.78)。与无病理反应相比,主要病理反应(HR 0.66,95% CI 0.44 - 0.99)与OS相关,而部分病理反应(HR 0.82,95% CI 0.57 - 1.19)与OS无关。病理反应而非形态学反应和RECIST与早期复发显著相关(P < 0.001),13/58(22%)主要反应患者、29/61(48%)部分反应患者和51/88(58%)无反应患者出现早期复发。
我们的结果表明,RECIST而非形态学反应对OS具有预后价值。在适合局部治疗的患者中,RECIST和形态学反应均与早期复发无关。病理反应与早期复发相关,但仅在术后可得。因此,需要新的术前参数来预测早期复发并避免潜在的无效肝脏手术。