Le Quang Dinh, Le Nhan Quang, Quach Duc Trong
Department of Internal Medicine University of Medicine and Pharmacy at Ho Chi Minh City Ho Chi Minh City Vietnam.
GI Endoscopy Department University Medical Center Ho Chi Minh City Ho Chi Minh City Vietnam.
JGH Open. 2024 Dec 12;8(12):e70075. doi: 10.1002/jgh3.70075. eCollection 2024 Dec.
Underwater endoscopic mucosal resection (UEMR) has emerged as a promising alternative to conventional endoscopic mucosal resection (CEMR) for the treatment of colorectal laterally spreading tumors (LSTs). This study aimed to compare the efficacy and safety of UEMR and CEMR in managing LSTs measuring 10-30 mm.
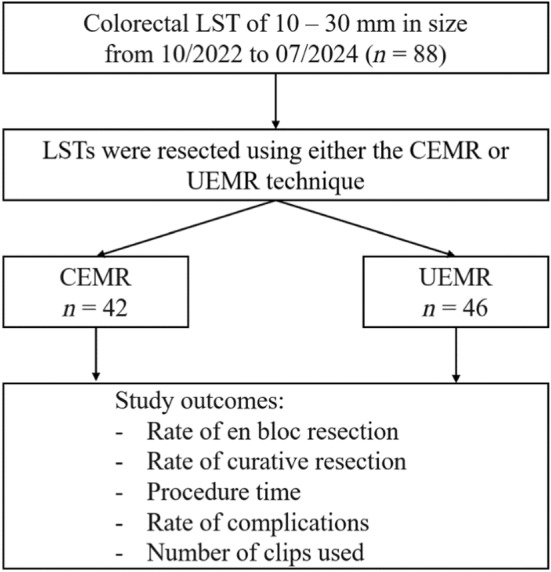
A post hoc analysis was performed on 88 patients with 88 colorectal LSTs, who were randomly assigned to two treatment groups: 42 with CEMR and 46 with UEMR. The primary outcome was the rate of R0 resection, defined as the absence of neoplastic cells at the resection margin. The secondary outcomes included en bloc resection rates, procedure times, and postprocedural complications. The data were analyzed via chi-square tests, tests, and the Mann-Whitney U test where appropriate.
No significant difference was found in the R0 resection rate between UEMR and CEMR. However, UEMR achieved a significantly higher en bloc resection rate, particularly for LSTs ranging from 20 to 30 mm (42.9% for CEMR vs. 100% for UEMR; = 0.009). Additionally, UEMR resulted in a shorter median procedure time (85.0 s for UEMR vs. 207.5 s for CEMR; < 0.001). There was no significant difference in bleeding complications or the number of clips used between the two groups.
Compared with CEMR, UEMR offers a higher en bloc resection rate and a shorter procedure time, particularly for larger lesions, without increasing the risk of complications. UEMR should be considered a preferred option for managing colorectal LSTs, especially those measuring 20-30 mm.
水下内镜黏膜切除术(UEMR)已成为治疗结直肠侧向发育型肿瘤(LST)的一种有前景的替代传统内镜黏膜切除术(CEMR)的方法。本研究旨在比较UEMR和CEMR治疗直径10 - 30毫米LST的疗效和安全性。
对88例患有88个结直肠LST的患者进行事后分析,这些患者被随机分为两个治疗组:42例行CEMR,46例行UEMR。主要结局是R0切除率,定义为切缘无肿瘤细胞。次要结局包括整块切除率、手术时间和术后并发症。数据在适当情况下通过卡方检验、t检验和曼-惠特尼U检验进行分析。
UEMR和CEMR的R0切除率无显著差异。然而,UEMR的整块切除率显著更高,特别是对于直径20至30毫米的LST(CEMR为42.9%,UEMR为100%;P = 0.009)。此外,UEMR的中位手术时间更短(UEMR为85.0秒,CEMR为207.5秒;P < 0.001)。两组在出血并发症或使用夹子数量方面无显著差异。
与CEMR相比,UEMR具有更高的整块切除率和更短的手术时间,特别是对于较大病变,且不增加并发症风险。UEMR应被视为治疗结直肠LST的首选方法,尤其是那些直径为20 - 30毫米的病变。