Nagase Takahiko, Kikuchi Takafumi, Akai Shun, Himeno Masafumi, Ooyama Ryo, Yoshida Yoshinori, Yoshino Chiyo, Nishida Takafumi, Tanaka Takahisa, Ishino Mitsunori, Kato Ryuichi, Kuwada Masao
Department of Cardiology Higashiyamato Hospital Tokyo Japan.
J Arrhythm. 2024 Oct 14;40(6):1432-1441. doi: 10.1002/joa3.13148. eCollection 2024 Dec.
Differences in predictability of ablation success for premature ventricular contractions (PVCs) between earliest isochronal map area (EIA), local activation time (LAT) differences on unipolar and bipolar electrograms (⊿LAT), LAT prematurity on bipolar electrograms (LAT), and unipolar morphology of QS or Q pattern remain unclear. We verified multiple statistical predictabilities of those indicators of ablation success on mapped cardiac surface.
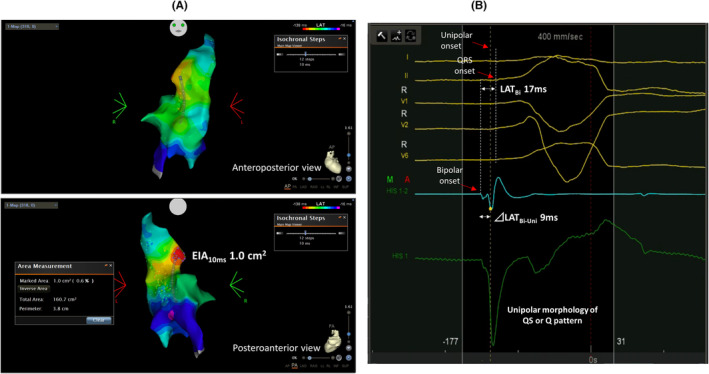
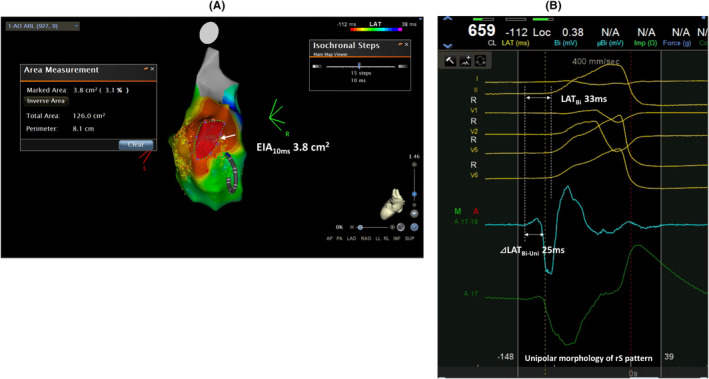
Thirty-five patients with multiple PVCs underwent catheter ablation after LAT mapping using multipolar mapping catheters with unipolar-based annotation. Patients were divided into success and failure groups based on ablation success on mapped cardiac surfaces. Discrimination ability, reclassification table, calibration plots, and decision curve analysis of 10 ms EIA (EIA), ⊿LAT, and LAT were validated. Unipolar morphology was compared between success and failure groups.
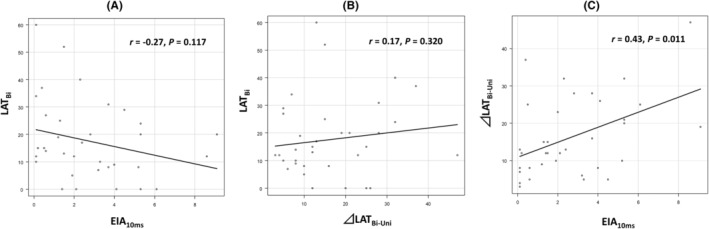
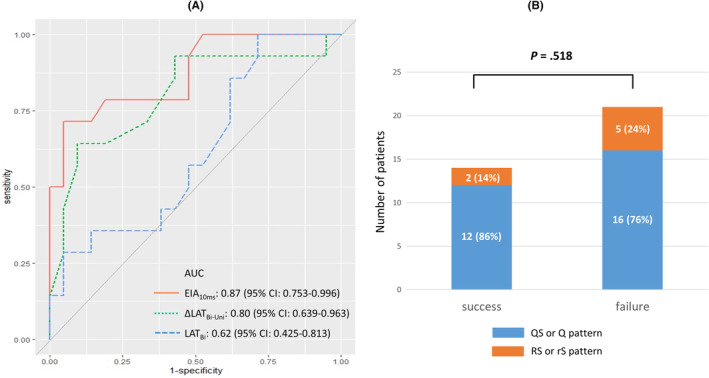
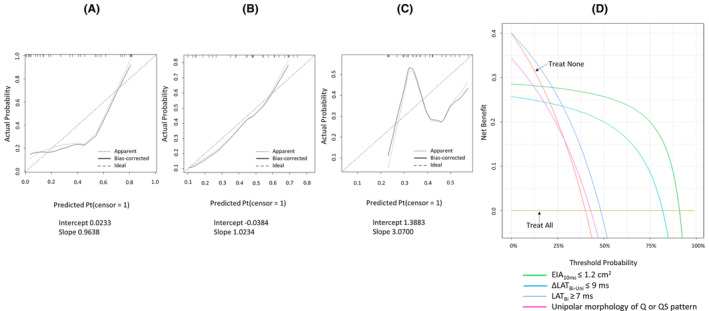
Right ventricular outflow tract, aortic cusp, and left ventricle were mapped in 17, 10, and 8 patients, respectively. In 14/35 (40%) patients, successful ablation was performed on mapped cardiac surfaces. Area under the curve of receiver-operating characteristic curve of EIA, ⊿LAT, and LAT were 0.874, 0.801, and 0.650, respectively (EIA vs. LAT, =.014; ⊿LAT vs. LAT, =.278; EIA vs. ⊿LAT, =.464). EIA and ⊿LAT demonstrated better predictability, calibration, and clinical utility on reclassification table, calibration plots, and decision curve analysis than LAT. Unipolar morphology of QS or Q pattern did not correlate with ablation success ( =.518).
EIA and ⊿LAT more accurately predict ablation success for PVCs on mapped cardiac surfaces than LAT and unipolar morphology.
在最早等时图区域(EIA)、单极和双极电图上的局部激动时间(LAT)差异(⊿LAT)、双极电图上的LAT提前程度(LAT)以及QS或Q波型的单极形态之间,室性早搏(PVC)消融成功率的可预测性差异尚不清楚。我们验证了这些消融成功指标在心脏表面标测上的多种统计可预测性。
35例患有多个PVC的患者在使用基于单极标注的多极标测导管进行LAT标测后接受导管消融。根据心脏表面标测的消融成功情况将患者分为成功组和失败组。对10毫秒EIA(EIA)、⊿LAT和LAT的辨别能力、重新分类表、校准图和决策曲线分析进行了验证。比较了成功组和失败组之间的单极形态。
分别对17例、10例和8例患者的右心室流出道、主动脉瓣尖和左心室进行了标测。在14/35(40%)的患者中,在心脏表面标测上进行了成功的消融。EIA、⊿LAT和LAT的受试者操作特征曲线下面积分别为0.874、0.801和0.650(EIA与LAT比较,P = 0.014;⊿LAT与LAT比较,P = 0.278;EIA与⊿LAT比较,P = 0.464)。在重新分类表、校准图和决策曲线分析方面,EIA和⊿LAT比LAT表现出更好的可预测性、校准和临床实用性。QS或Q波型的单极形态与消融成功无关(P = 0.518)。
在心脏表面标测上,EIA和⊿LAT比LAT和单极形态更准确地预测PVC的消融成功。