Yamada Mayu, Ueno Katsumi, Kojima Yoshinobu, Watanabe Mitsuru, Morita Norihiko
Department of Cardiology, Matsunami General Hospital, Kasamatsu, Gifu 501-6062, Japan.
Department of Rheumatology, Daido Hospital, 9 Hakusui, Minami, Nagoya City, Aichi 457-8511, Japan.
Eur Heart J Case Rep. 2024 Sep 10;8(10):ytae492. doi: 10.1093/ehjcr/ytae492. eCollection 2024 Oct.
Although coronary artery involvement in patients with IgG4-related disease (IgG4-RD) is rare, emergency revascularization is recommended for managing acute coronary syndrome. However, coronary aneurysm formation and stent migration after sirolimus-eluting stent implantation have been reported for this disease. Thus, new treatment modalities are warranted for the management of coronary artery disease in this vasculitis.
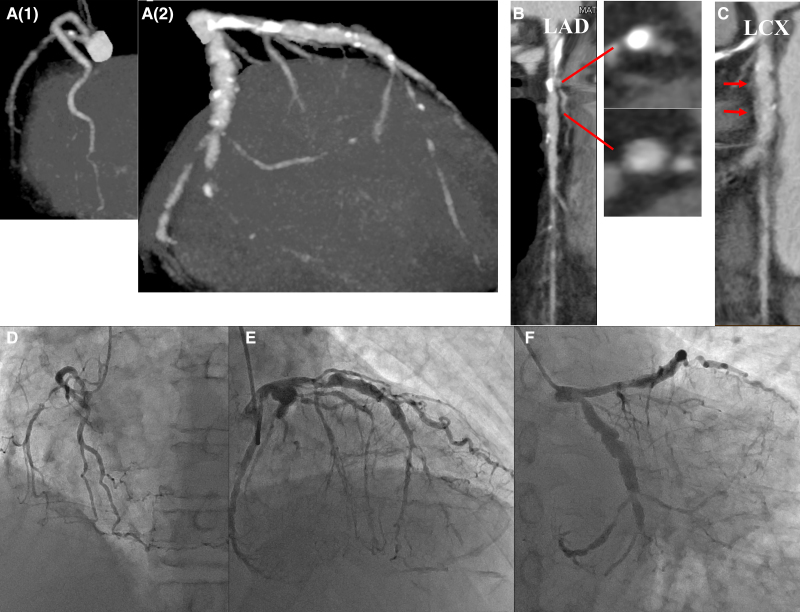
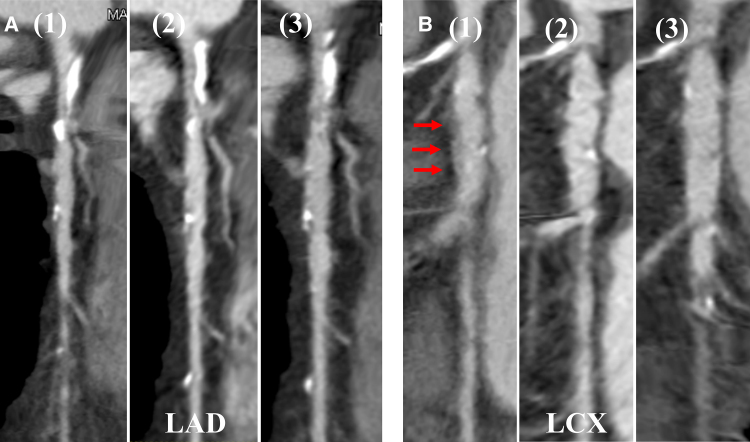
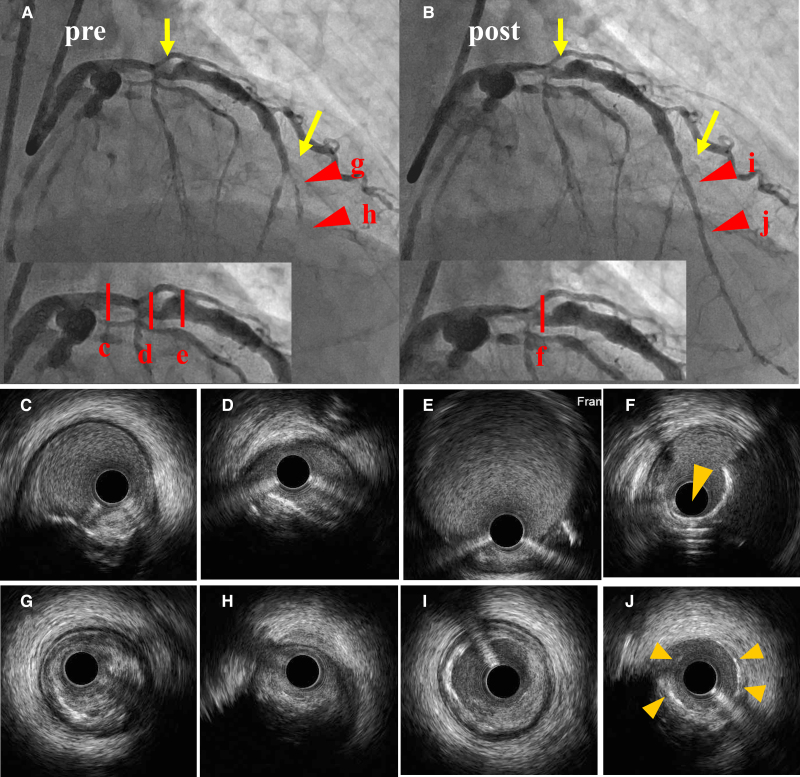
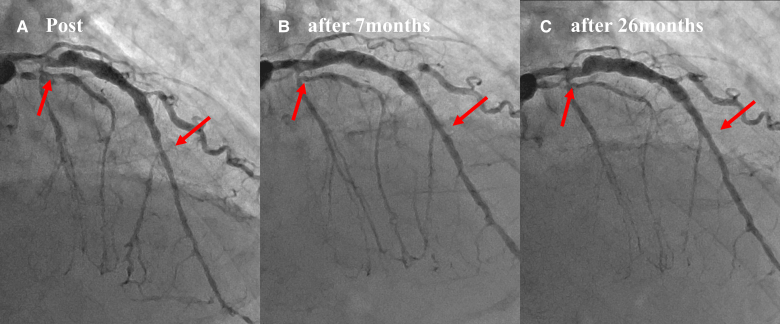
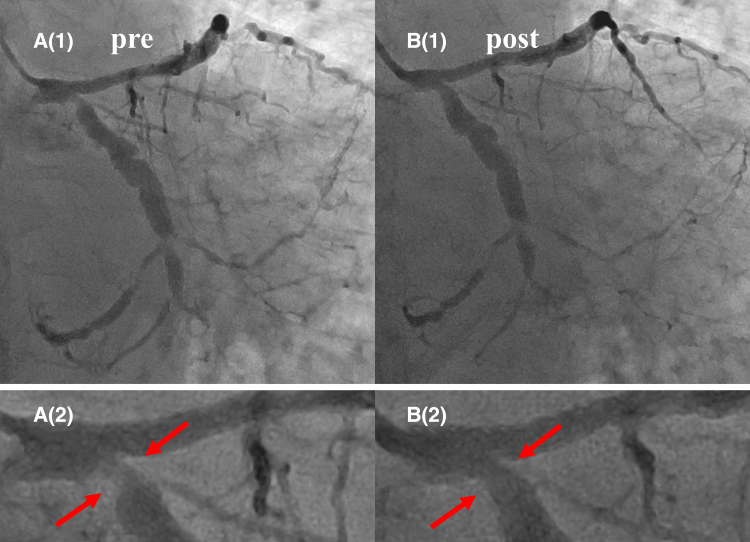
A 70-year-old male who experienced progressive chest discomfort for 1 month underwent cardiac examination. Coronary computed tomography angiography (CCTA) revealed right coronary artery hypoplasia, coronary artery aneurysm with severely calcified stenosis in the proximal left anterior descending artery (LAD), and subtotal obstruction in the mid-LAD. The left circumflex artery (LCX) also had stenosis and dilated lesions. Additionally, diffuse perivascular soft tissue thickening was observed in the mid-LCX. The percutaneous coronary intervention was performed for the proximal- and mid-LAD lesions. Rotational atherectomy with low-pressure drug-coated balloon (DCB) dilation was considered for these lesions owing to suspicion of vasculitis. The patient was later diagnosed with Sjögren's syndrome and IgG4-RD overlap syndrome. Oral steroids and immunosuppressive drugs were initiated. In a follow-up at 7 and 26 months, late lumen enlargement was observed in the treated area of the LAD, without enlargement of the adjacent aneurysm. CCTA performed after 26 months revealed resolution of the diffuse perivascular soft tissue thickening in the mid-LCX.
To our knowledge, this is the first case report demonstrating favourable outcomes for treatment of a coronary artery lesion attributed to IgG4-RD with DCB, leaving nothing implanted in the coronary artery tree.
尽管IgG4相关性疾病(IgG4-RD)患者的冠状动脉受累情况罕见,但对于急性冠状动脉综合征的治疗,仍建议进行紧急血运重建。然而,已有报道称该疾病在西罗莫司洗脱支架植入后会出现冠状动脉瘤形成和支架迁移。因此,需要新的治疗方式来管理这种血管炎中的冠状动脉疾病。
一名70岁男性,因进行性胸部不适1个月接受心脏检查。冠状动脉计算机断层扫描血管造影(CCTA)显示右冠状动脉发育不全,左前降支近端严重钙化狭窄的冠状动脉瘤,以及左前降支中段次全阻塞。左旋支(LCX)也有狭窄和扩张性病变。此外,在LCX中段观察到弥漫性血管周围软组织增厚。对左前降支近端和中段病变进行了经皮冠状动脉介入治疗。由于怀疑血管炎,考虑对这些病变采用旋磨术联合低压药物涂层球囊(DCB)扩张。该患者后来被诊断为干燥综合征和IgG4-RD重叠综合征。开始口服类固醇和免疫抑制药物。在7个月和26个月的随访中,左前降支治疗区域出现晚期管腔扩大,相邻动脉瘤未扩大。26个月后进行的CCTA显示LCX中段弥漫性血管周围软组织增厚消退。
据我们所知,这是第一例报告,证明使用DCB治疗归因于IgG4-RD的冠状动脉病变取得了良好效果,冠状动脉内未植入任何东西。