Sung Hyuna, Siegel Rebecca L, Laversanne Mathieu, Jiang Chenxi, Morgan Eileen, Zahwe Mariam, Cao Yin, Bray Freddie, Jemal Ahmedin
Surveillance and Health Equity Science, American Cancer Society, Atlanta, GA, USA.
Surveillance and Health Equity Science, American Cancer Society, Atlanta, GA, USA.
Lancet Oncol. 2025 Jan;26(1):51-63. doi: 10.1016/S1470-2045(24)00600-4. Epub 2024 Dec 12.
Previous studies have shown that colorectal cancer incidence is increasing among younger adults (aged <50 years) in multiple high-income western countries in contrast with stabilising or decreasing trends in incidence in older adults (aged ≥50 years). This study aimed to investigate contemporary colorectal cancer incidence trends in younger adults versus older adults.
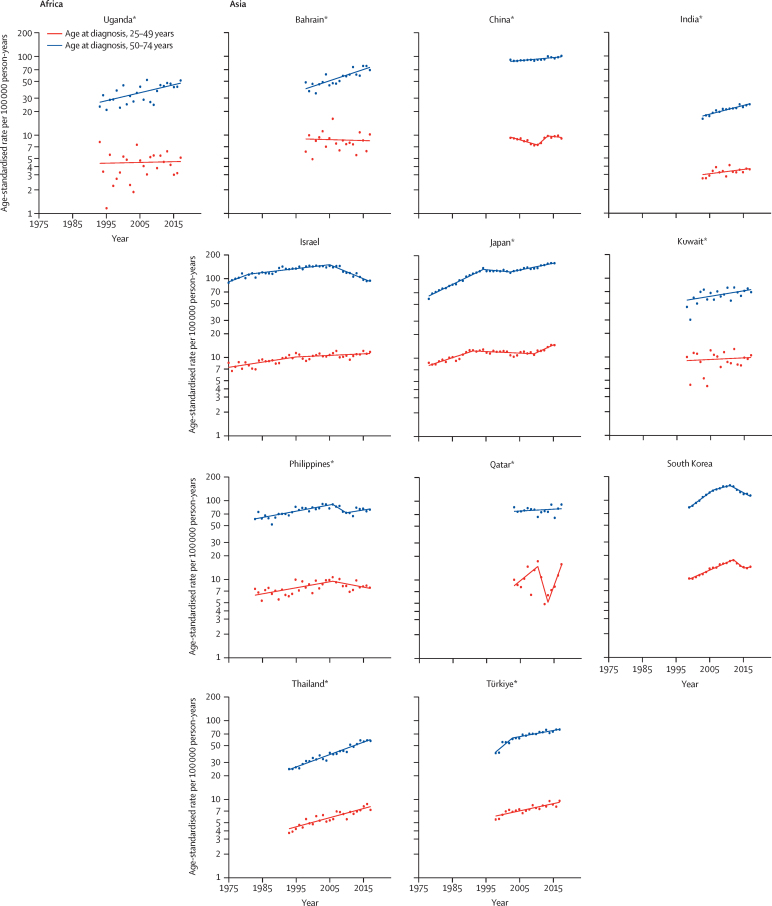
Colorectal cancer incidence data, including year of diagnosis, sex, and 5-year age group for 50 countries and territories, were extracted from the WHO-International Agency for Research on Cancer Cancer Incidence in Five Continents Plus database. The Human Development Index 2022 was retrieved from the United Nations Development Programme and grouped into very high (>0·80), high (0·70-0·79), medium (0·55-0·69), and low (<0·55) categories. Age-standardised incidence rates (ASR) per 100 000 person-years of early-onset (diagnosed between ages 25 to 49 years) and late-onset (diagnosed between ages 50 to 74 years) colorectal cancer (ICD 10th revision, C18-20), diagnosed between 1943-2003 and 2015-17, were calculated using the direct method and Segi-Doll world standard population). The primary study objective was to examine contemporary colorectal cancer incidence trends in younger adults versus older adults using data until 2017 from 50 countries and territories. Temporal trends were visualised and quantified with joinpoint regression, stratified by age at diagnosis (25-49 years or 50-74 years). Average annual percentage changes (AAPC) were estimated.
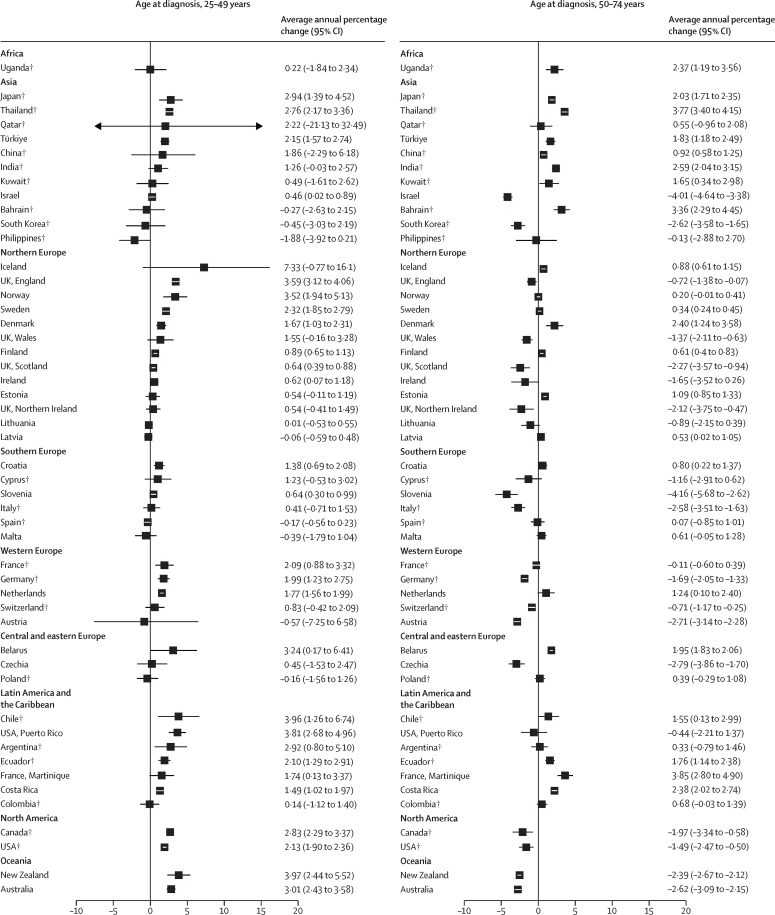
In the most recent 5 years (2013-17 for all countries analysed, except for Japan [2011-15], Spain [2012-16], and Costa Rica [2012-16]), the incidence rate of early-onset colorectal cancer was highest in Australia (ASR 16·5 [95% CI 16·1-16·9]), the USA (Puerto Rico; 15·2 [14·2-16·2]), New Zealand (14·8 [14·0-15·6]), the USA (14·8 [14·7-14·9]), and South Korea (14·3 [14·0-14·5]) and lowest in Uganda (4·4 [3·6-5·2]) and India (3·5 [3·3-3·7]). The highest incidence rates among older adults were found in the Netherlands (168·4 [166·9-170·0]) and Denmark (158·3 [155·8-160·9]) and the lowest were in Uganda (45·9 [38·5-51·4]) and India (23·5 [22·8-24·3]). In terms of AAPC, in the most recent 10 years, incidence rates of early-onset colorectal cancer were stable in 23 countries, but increased in 27 countries with the greatest annual increases in New Zealand (AAPC 3·97% [95% CI 2·44-5·52]), Chile (3·96% [1·26-6·74]), Puerto Rico (3·81% [2·68-4·96]), and England (3·59% [3·12-4·06]). 14 of the 27 countries and territories showed either stable (Argentina, France, Ireland, Norway, and Puerto Rico) or decreasing (Australia, Canada, Germany, Israel, New Zealand, Slovenia, England, Scotland, and the USA) trends in older adults. For the 13 countries with increasing trends in both age groups, the average annual percentage increase in younger compared to older adults was higher in Chile, Japan, Sweden, the Netherlands, Croatia, and Finland; lower in Thailand, France (Martinique), Denmark, and Costa Rica; and similar in Türkiye, Ecuador, and Belarus. The rise in early-onset colorectal cancer was faster among men than women in Chile, Puerto Rico, Argentina, Ecuador, Thailand, Sweden, Israel, and Croatia, whereas faster increase among women compared to men was in England, Norway, Australia, Türkiye, Costa Rica, and Scotland.
Early-onset colorectal cancer incidence rates are rising in 27 of 50 countries and territories examined, with the rise either exclusive to early-onset disease or faster than the increase in older adults in 20 of the 27 countries. The findings underscore the need for intensified efforts to identify factors driving these trends and increase awareness to help facilitate early detection.
Intramural Research Program of the American Cancer Society, Cancer Grand Challenges, and National Institutes of Health.
先前的研究表明,在多个西方高收入国家,较年轻成年人(年龄<50岁)的结直肠癌发病率呈上升趋势,而较年长成年人(年龄≥50岁)的发病率则呈稳定或下降趋势。本研究旨在调查较年轻与较年长成年人当代结直肠癌发病率趋势。
从世界卫生组织国际癌症研究机构的《五大洲癌症发病率加》数据库中提取了50个国家和地区的结直肠癌发病率数据,包括诊断年份、性别和5岁年龄组。从联合国开发计划署获取了2022年人类发展指数,并将其分为非常高(>0.80)、高(0.70 - 0.79)、中(0.55 - 0.69)和低(<0.55)四类。采用直接法和Segi - Doll世界标准人口,计算了1943 - 2003年和2015 - 2017年期间每10万人年早发性(25至49岁诊断)和晚发性(50至74岁诊断)结直肠癌(国际疾病分类第10版,C18 - 20)的年龄标准化发病率(ASR)。主要研究目标是利用50个国家和地区截至2017年的数据,研究较年轻与较年长成年人当代结直肠癌发病率趋势。通过连接点回归对时间趋势进行可视化和量化,按诊断年龄(25 - 49岁或50 - 74岁)分层。估计平均年度百分比变化(AAPC)。
在最近五年(所有分析国家为2013 - 2017年,日本为2011 - 2015年,西班牙为2012 - 2016年,哥斯达黎加为2012 - 2016年),早发性结直肠癌发病率在澳大利亚最高(ASR 16.5 [95% CI 16.1 - 16.9])、美国(波多黎各;15.2 [14.2 - 16.2])、新西兰(14.8 [14.0 - 15.6])、美国(14.8 [14.7 - 14.9])和韩国(14.3 [14.0 - 14.5]),在乌干达最低(4.4 [3.6 - 5.2])和印度(3.5 [3.3 - 3.7])。较年长成年人中发病率最高的是荷兰(168.4 [166.9 - 170.0])和丹麦(158.3 [155.8 - 160.9]),最低的是乌干达(45.9 [38.5 - 51.4])和印度(23.5 [22.8 - 24.3])。就AAPC而言,在最近十年中,23个国家早发性结直肠癌发病率稳定,但27个国家上升,其中新西兰年度增幅最大(AAPC 3.97% [95% CI 2.44 - 5.52])、智利(3.96% [1.26 - 6.74])、波多黎各(3.81% [2.68 - 4.96])和英格兰(3.59% [3.12 - 4.06])。27个国家和地区中有14个在较年长成年人中呈稳定(阿根廷、法国、爱尔兰、挪威和波多黎各)或下降(澳大利亚、加拿大、德国、以色列、新西兰、斯洛文尼亚、英格兰、苏格兰和美国)趋势。在两个年龄组均呈上升趋势的13个国家中,智利、日本、瑞典、荷兰、克罗地亚和芬兰较年轻成年人相比较年长成年人的平均年度百分比增幅更高;泰国、法国(马提尼克岛)、丹麦和哥斯达黎加较低;土耳其、厄瓜多尔和白俄罗斯相近。在智利、波多黎各、阿根廷、厄瓜多尔、泰国、瑞典、以色列和克罗地亚,早发性结直肠癌男性发病率上升速度快于女性,而在英格兰、挪威、澳大利亚、土耳其、哥斯达黎加和苏格兰,女性发病率上升速度快于男性。
在所研究的50个国家和地区中,27个早发性结直肠癌发病率呈上升趋势,其中20个国家早发性疾病发病率单独上升或上升速度快于较年长成年人。这些发现强调需要加大力度确定推动这些趋势的因素,并提高认识以促进早期检测。
美国癌症协会、癌症重大挑战和美国国立卫生研究院的内部研究项目。