Cruz-Diaz Wagner Eduardo, Paitan Victor, Medina Jersinho, Flores Raymundo, Haro-Varas Juan, Mantilla Raul, Castro-Oliden Victor
Department of Oncology, Instituto Nacional de Enfermedades Neoplásicas, Lima 15038, Perú.
Department of Pathology, Instituto Nacional de Enfermedades Neoplásicas, Lima 15038, Perú.
World J Gastrointest Oncol. 2024 Dec 15;16(12):4675-4684. doi: 10.4251/wjgo.v16.i12.4675.
Numerous studies have indicated that the temozolomide and capecitabine regimen (TEMCAP) exhibits a certain level of efficacy in treating advanced, well-differentiated gastroenteropancreatic neuroendocrine tumors (GEP-NET). However, published data from Peru are limited. We hypothesize that this regimen could be a viable therapeutic option for advanced GEP-NET in the Peruvian population.
To evaluate overall survival (OS) in patients diagnosed with advanced GEP-NET treated with TEMCAP at the Instituto Nacional de Enfermedades Neoplásicas (INEN) in Lima-Perú.
A retrospective review was conducted to identify patients with GEP-NEN treated with the TEMCAP regimen between 2011 and 2021 at the INEN. A total of thirty-eight patients were included in the final analysis: Thirty-five received TEMCAP as a first-line treatment, and three as a second-line treatment. The primary objective was to evaluate OS. The efficacy and safety of TEMCAP were assessed until the occurrence of unacceptable toxicity or disease progression. Survival outcomes were estimated using the Kaplan-Meier method.
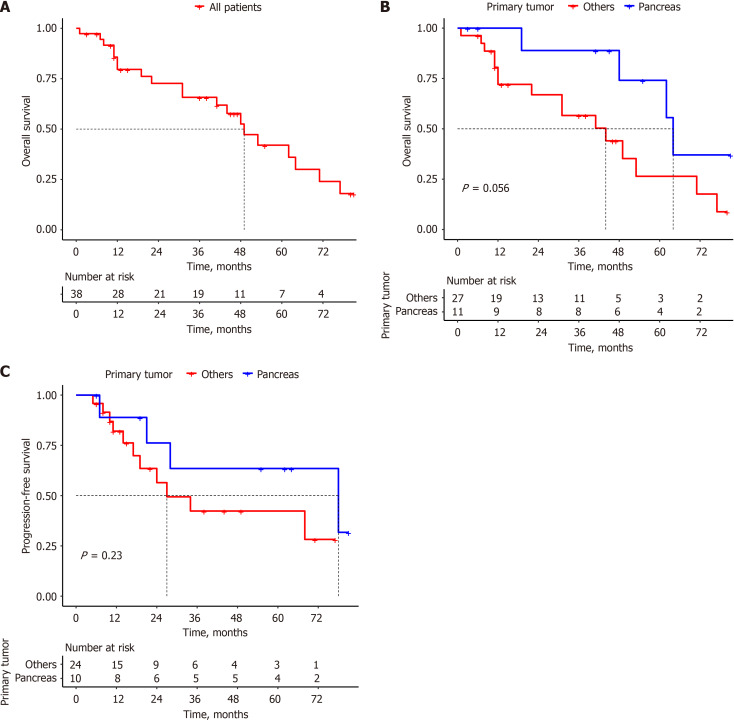
The median age of the patients was 52 years (range 24-77 years), and 53.3% were female. The most common symptoms at diagnosis were abdominal pain in 31 patients (81.6%). Primary tumors included 12 in the rectum (31.6%), 11 in the pancreas (28.9%), 3 in the ileum (7.9%), 2 in the mesentery (5.3%), 2 in the small intestine (5.3%), 1 in the appendix (2.6%), 1 in the stomach (2.6%) and 6 cases of liver metastasis of unknown primary (15.8%). Five were neuroendocrine tumors (NET) G1 (13.2%), 33 were NET G2 (86.8%), five had Ki67 < 3% (13.2%), and 33 had Ki67 between 3% and 20% (86.8%). TEMCAP was administered to 35 (92.1%) patients as first-line treatment. OS at 12, 36, and 60 months was estimated in 80%, 66%, and 42%, respectively, with a median OS of 49 months.
TEMCAP therapy is a viable first-line option regarding efficacy and tolerability in areas where standard therapy is inaccessible.
大量研究表明,替莫唑胺和卡培他滨方案(TEMCAP)在治疗晚期、高分化胃肠胰神经内分泌肿瘤(GEP-NET)方面显示出一定疗效。然而,来自秘鲁的已发表数据有限。我们推测该方案可能是秘鲁人群晚期GEP-NET的一种可行治疗选择。
评估在秘鲁利马国家肿瘤研究所(INEN)接受TEMCAP治疗的晚期GEP-NET患者的总生存期(OS)。
进行一项回顾性研究,以确定2011年至2021年期间在INEN接受TEMCAP方案治疗的GEP-NEN患者。最终分析共纳入38例患者:35例接受TEMCAP作为一线治疗,3例作为二线治疗。主要目的是评估总生存期。评估TEMCAP的疗效和安全性直至出现不可接受的毒性或疾病进展。使用Kaplan-Meier方法估计生存结局。
患者的中位年龄为52岁(范围24 - 77岁),53.3%为女性。诊断时最常见的症状是31例患者出现腹痛(81.6%)。原发肿瘤包括直肠12例(31.6%)、胰腺11例(28.9%)、回肠3例(7.9%)、肠系膜2例(5.3%)、小肠2例(5.3%)、阑尾1例(2.6%)、胃1例(2.6%)以及6例原发灶不明的肝转移(15.8%)。5例为神经内分泌肿瘤(NET)G1(13.2%),33例为NET G2(86.8%),5例Ki67<3%(13.2%),33例Ki67在3%至20%之间(86.8%)。35例(92.1%)患者接受TEMCAP作为一线治疗。12个月、36个月和60个月时的总生存期估计分别为80%、66%和42%,中位总生存期为49个月。
在无法获得标准治疗的地区,TEMCAP治疗在疗效和耐受性方面是一种可行的一线选择。