Nogueira Daniel Silva, Lage Luís Alberto de Pádua Covas, Reichert Cadiele Oliana, Culler Hebert Fabrício, de Freitas Fábio Alessandro, Mendes João Antônio Tavares, Gouveia Ana Carolina Maia, Costa Renata de Oliveira, Ferreira Cristiane Rúbia, Maximino Jéssica Ruivo, Bydlowski Sérgio Paulo, Murga Zamalloa Carlos Alejandro, Rocha Vanderson, Levy Débora, Pereira Juliana
Department of Hematology, Hemotherapy and Cell Therapy, Faculty of Medicine, University of Sao Paulo (FM-USP), Sao Paulo 05508-090, Brazil.
Laboratory of Medical Investigation in Pathogenesis and Directed Therapy in Onco-Immuno-Hematology (LIM-31), University of Sao Paulo (FM-USP), Sao Paulo 05508-090, Brazil.
Cancers (Basel). 2024 Nov 22;16(23):3914. doi: 10.3390/cancers16233914.
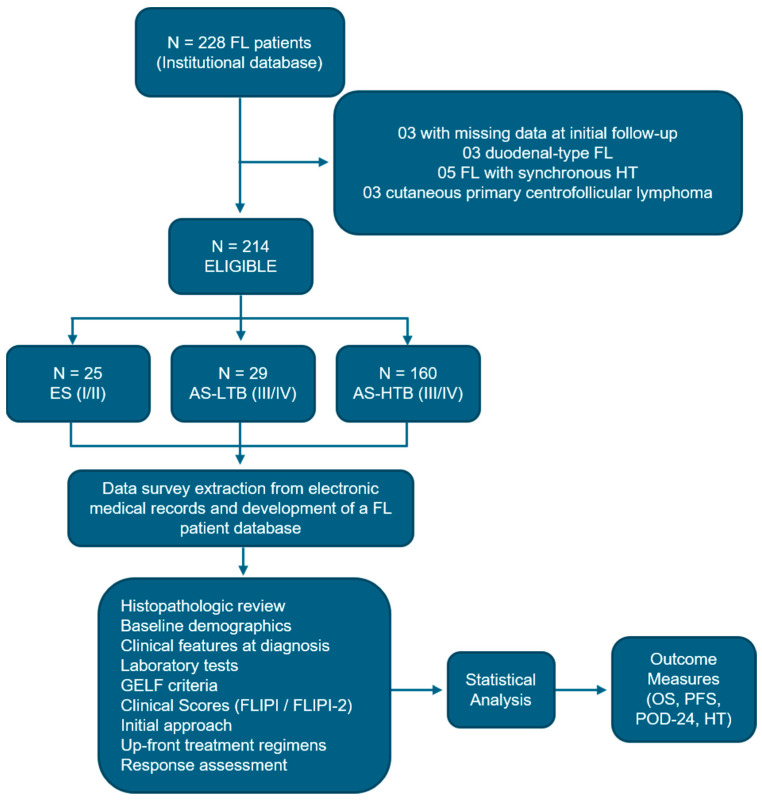
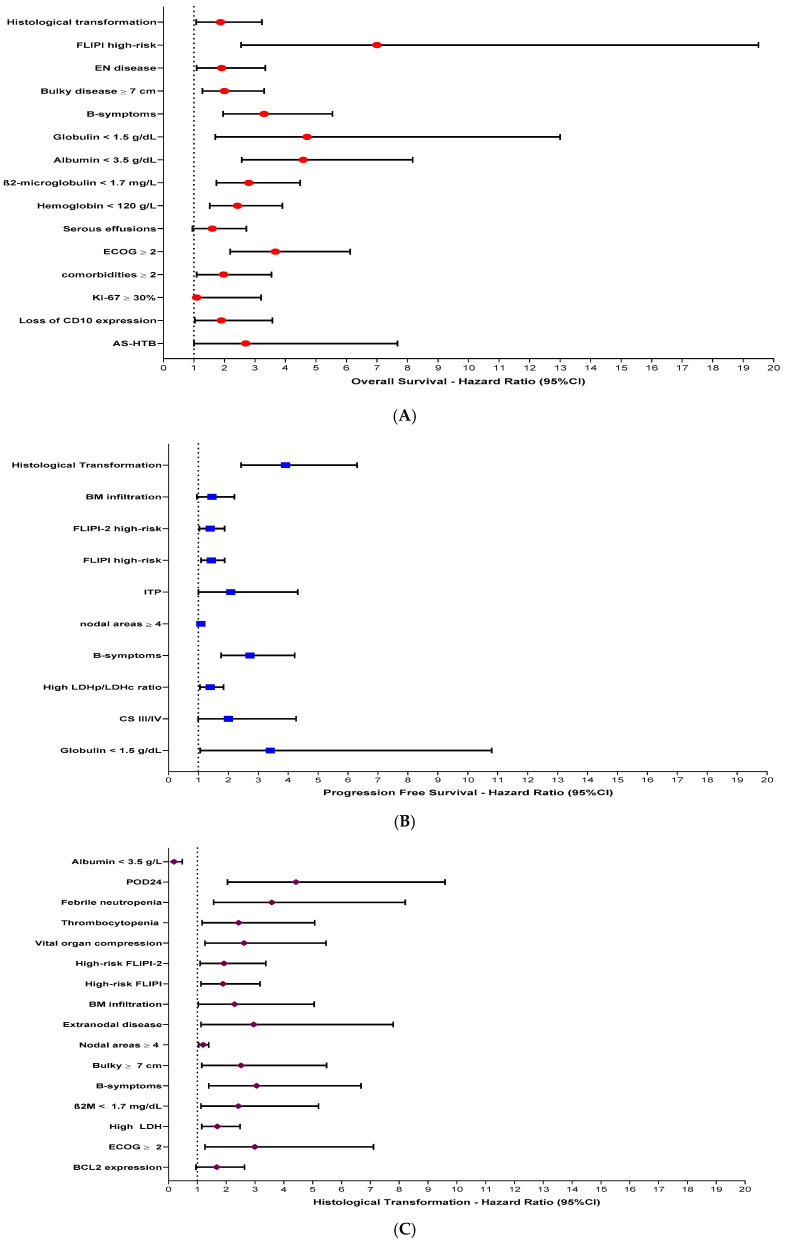
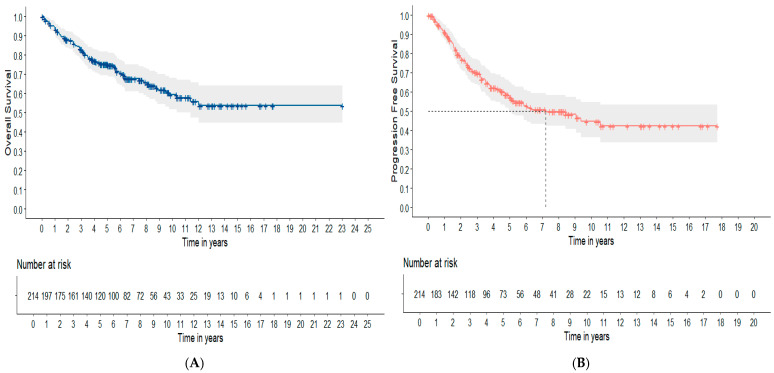
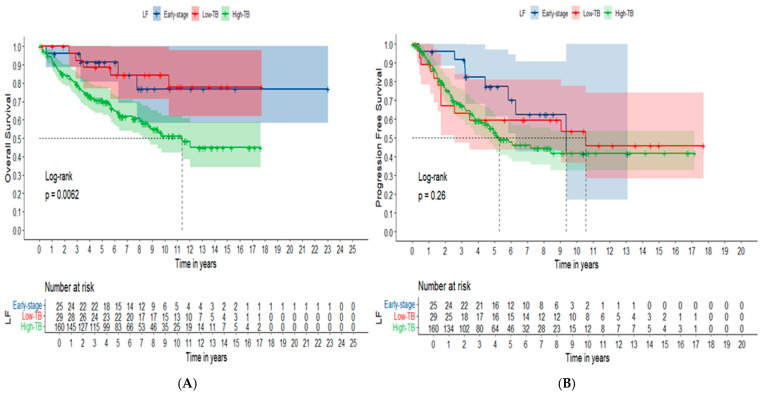
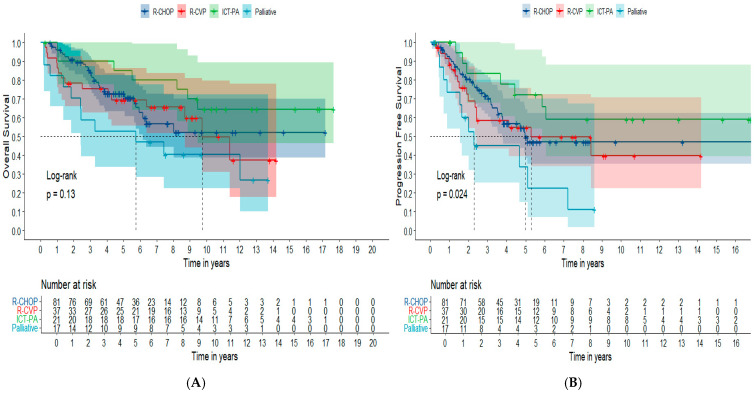
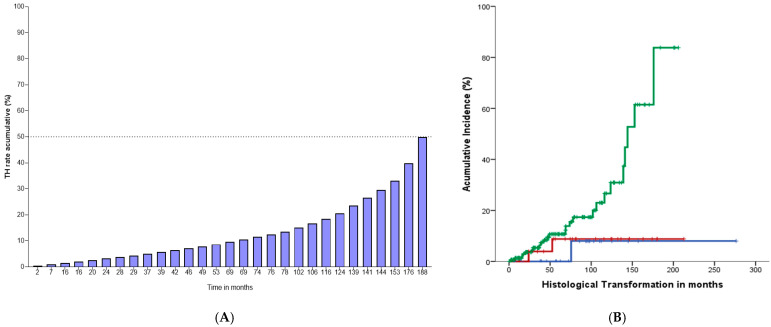
Clinical staging (CS) and tumor burden (TB) play a significant role in FL prognosis and direct its up-front therapy. The aim of this study is to report prognostic factors and clinical outcomes in newly-diagnosed FL patients stratified according to CS and TB in early-stage (ES) disease, advanced-stage with low tumor burden (AS-LTB) and advanced-stage with high tumor burden (AS-HTB). Two hundred fourteen patients with FL grades 1-3A had baseline clinical characteristics and outcomes assessed. Survival according to up-front immunochemotherapeutic (ICT) regimens was assessed in the AS-HTB subgroup. Independent predictors for OS, PFS, POD-24, and Histological Transformation (HT) were identified. Seventy-five percent of cases were categorized as AS-HTB, 13.5% as AS-LTB and 11.5% as ES. With a median follow-up of 8.15 years, the estimated 5-year OS and PFS were 75.4% and 57.2%, respectively. OS, but not PFS was markedly decreased in AS-HTB FL patients compared to ES and AS-LTB cases. POD-24 rate was 21.7% and overall mortality rate was 38.7% during the entire follow-up. The annual cumulative rate of HT to high-grade B-cell lymphoma (HGBCL) was 0.5%, and higher in AS-HTB cases, in comparison to ES and AS-LTB. Considering patients with AS-HTB there were no differences in clinical outcomes among cases submitted to ICT based on R-CHOP, R-CVP and regimens containing purine analogs. Additionally, ECOG ≥ 2, hypoalbuminemia, B-symptoms and HT were independently associated with poor survival. High content of centro-blasts (grade 3A), involvement of ≥3 nodal sites by FL and rituximab omission in up-front therapy predicted POD-24. : FL has marked clinical-prognostic heterogeneity, translated into diverse CS and TB subcategories. Here, we demonstrated that FL patients classified as AS-HTB demonstrated decreased survival and higher rates of HT to HGBCL compared to ES and AS-LTB cases. Prognostic factors identified in our analysis may help to identify FL patients with higher-risk of HT and early-progression (POD-24).
临床分期(CS)和肿瘤负荷(TB)在滤泡性淋巴瘤(FL)的预后中起重要作用,并指导其初始治疗。本研究的目的是报告初诊FL患者的预后因素和临床结局,这些患者根据早期(ES)疾病、低肿瘤负荷晚期(AS-LTB)和高肿瘤负荷晚期(AS-HTB)的CS和TB进行分层。对214例1-3A级FL患者的基线临床特征和结局进行了评估。在AS-HTB亚组中评估了根据初始免疫化疗(ICT)方案的生存率。确定了总生存期(OS)、无进展生存期(PFS)、24个月无进展生存(POD-24)和组织学转化(HT)的独立预测因素。75%的病例归类为AS-HTB,13.5%为AS-LTB,11.5%为ES。中位随访8.15年,估计5年OS和PFS分别为75.4%和57.2%。与ES和AS-LTB病例相比,AS-HTB FL患者的OS显著降低,但PFS没有降低。在整个随访期间,POD-24率为21.7%,总死亡率为38.7%。向高级别B细胞淋巴瘤(HGBCL)的HT年累积率为0.5%,与ES和AS-LTB相比,AS-HTB病例中的发生率更高。对于AS-HTB患者,接受基于R-CHOP、R-CVP和含嘌呤类似物方案的ICT的病例之间的临床结局没有差异。此外,东部肿瘤协作组(ECOG)≥2、低白蛋白血症、B症状和HT与生存不良独立相关。中心母细胞含量高(3A级)、FL累及≥3个结外部位以及初始治疗中未使用利妥昔单抗可预测POD-24。FL具有明显的临床预后异质性,表现为不同的CS和TB亚类。在此,我们证明,与ES和AS-LTB病例相比,归类为AS-HTB的FL患者生存率降低,向HGBCL的HT率更高。我们分析中确定的预后因素可能有助于识别HT和早期进展(POD-24)风险较高的FL患者。