Chen Ying, Ma Zhu-Lin, Liu Fei, Wang Nan, Ma Yue-Yang, Guan Zi-An, Zhe Zhuang-Chuan, Xia Yun-Long, Dong Ying-Xue
Department of Cardiology, First Affiliated Hospital of Dalian Medical University, Dalian, China.
Front Physiol. 2024 Dec 2;15:1500159. doi: 10.3389/fphys.2024.1500159. eCollection 2024.
The relationship between conduction system pacing (CSP) and the incidence of atrial fibrillation (AF) in patients with heart failure and preserved ejection fraction (HFpEF) remains uncertain. This study aims to investigate the occurrence of atrial high-rate episodes (AHREs) following CSP in patients with HFpEF, in comparison to right ventricular pacing (RVP).
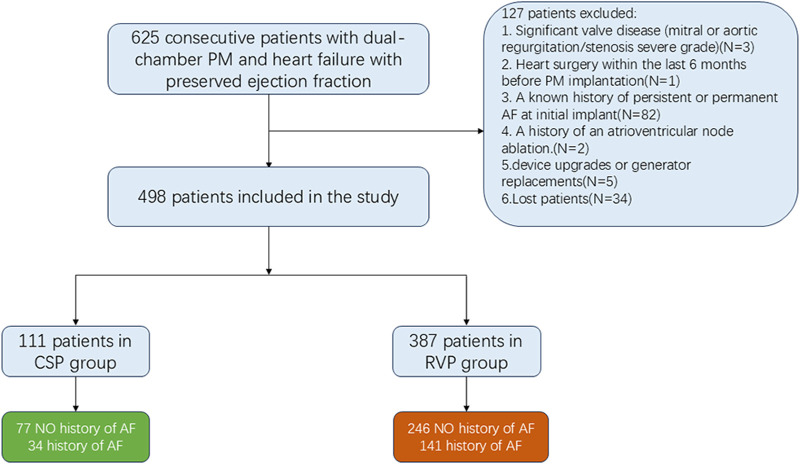
Patients with HFpEF who received dual-chamber pacemakers for atrioventricular block were retrospectively enrolled from January 2018 to January 2023. Both new-onset and progressive AHREs were recorded, along with other clinical data, including cardiac performance and lead outcomes.
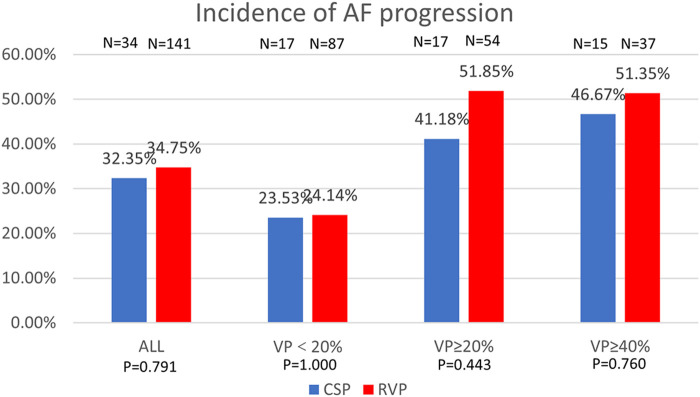
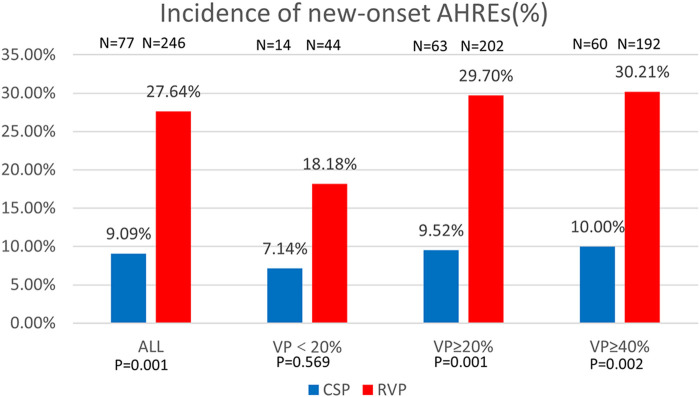
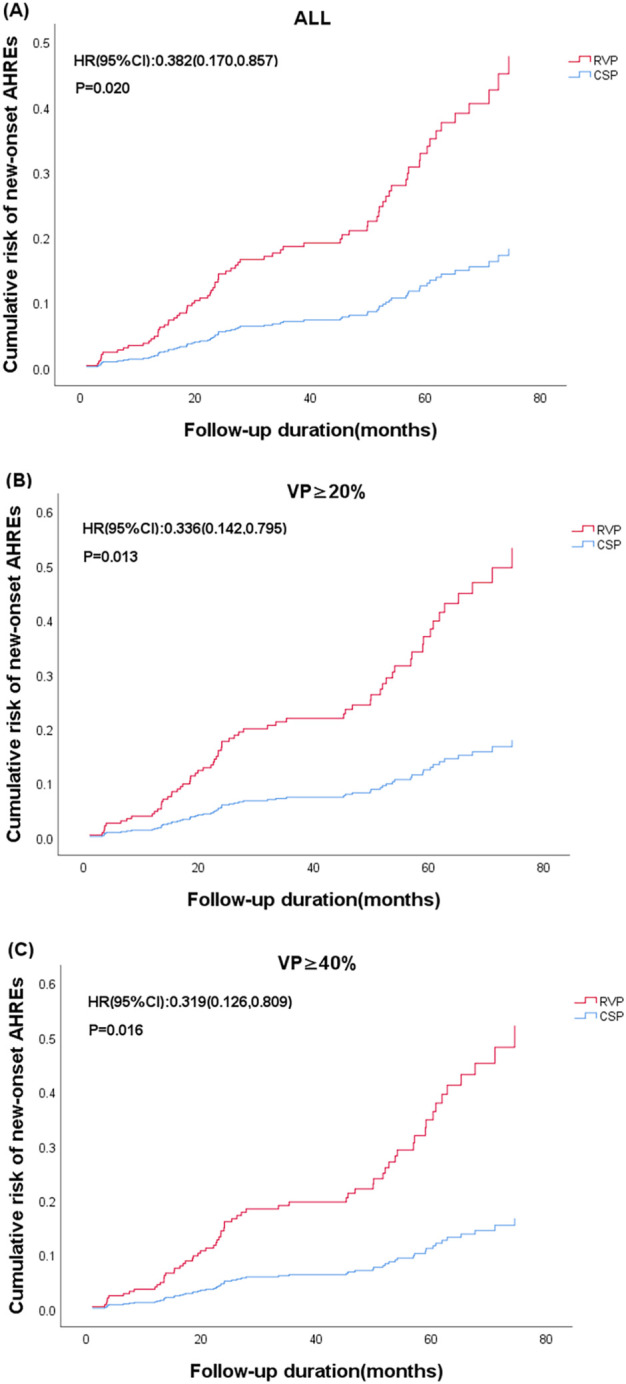
A total of 498 patients were enrolled, comprising 387 patients with RVP and 111 patients with CSP, with a follow-up duration of 44.42 ± 10.41 months. In patients without a prior history of AF, CSP was associated with a significantly lower incidence of new-onset AHREs when the percentage of ventricular pacing was ≥20% (9.52% vs. 29.70%, = 0.001). After adjusting for confounding factors, CSP exhibited a lower hazard ratio for new-onset AHREs compared to RVP (HR 0.336; [95% CI: 0.142-0.795]; = 0.013), alongside left atrial diameter (LAD) (HR 1.109; [95% CI: 1.048-1.173]; < 0.001). In patients with a history of AF, the progression of AHREs in CSP and RVP did not differ significantly (32.35% vs. 34.75%, = 0.791). Cardiac performance metrics, including left ventricular end-diastolic diameter (LVEDD) (49.09 ± 4.28 mm vs. 48.08 ± 4.72 mm; = 0.015), LAD (40.68 ± 5.49 mm vs. 39.47 ± 5.24 mm; = 0.001), and NYHA class (2.31 ± 0.46 vs. 1.59 ± 0.73; < 0.001), improved obviously following CSP, while LVEDD (48.37 ± 4.57 mm vs. 49.30 ± 5.32 mm; < 0.001), LAD (39.77 ± 4.58 mm vs. 40.83 ± 4.80 mm; < 0.001), NYHA class (2.24 ± 0.43 vs. 2.35 ± 0.83; = 0.018), and left ventricular ejection fraction (LVEF) (57.41 ± 2.42 vs. 54.24 ± 6.65; < 0.001) deteriorated after RVP.
Our findings suggest that CSP may be associated with improvements in cardiac performance and a reduction in new-onset AHREs compared to RVP in patients with HFpEF. However, prospective randomized trials are anticipated to confirm these potential benefits.
心力衰竭且射血分数保留(HFpEF)患者中,传导系统起搏(CSP)与心房颤动(AF)发生率之间的关系仍不明确。本研究旨在比较HFpEF患者中CSP与右心室起搏(RVP)后心房高率发作(AHREs)的发生情况。
回顾性纳入2018年1月至2023年1月因房室传导阻滞接受双腔起搏器治疗的HFpEF患者。记录新发和进展性AHREs以及其他临床数据,包括心脏功能和导线结局。
共纳入498例患者,其中387例接受RVP,111例接受CSP,随访时间为44.42±10.41个月。在无AF病史的患者中,当心室起搏百分比≥20%时,CSP与新发AHREs发生率显著降低相关(9.52%对29.70%,P = 0.001)。调整混杂因素后,与RVP相比,CSP新发AHREs的风险比更低(HR 0.336;[95%CI:0.142 - 0.795];P = 0.013),左心房直径(LAD)也是如此(HR 1.109;[95%CI:1.048 - 1.173];P < 0.001)。在有AF病史的患者中,CSP和RVP中AHREs的进展无显著差异(32.35%对34.75%,P = 0.791)。CSP后心脏功能指标,包括左心室舒张末期直径(LVEDD)(分别为49.09±4.28mm对48.08±4.72mm;P = 0.0十五年)、LAD(40.68±5.49mm对39.47±5.24mm;P = 0.001)和纽约心脏协会(NYHA)分级(2.31±0.46对1.59±0.73;P < 0.001)明显改善,而RVP后LVEDD(48.37±4.57mm对49.30±5.32mm;P < 0.001)、LAD(39.77±4.58mm对40.8三十 ±4.80mm;P < 0.001)、NYHA分级(2.24±0.43对2.35±0.83;P = 0.018)和左心室射血分数(LVEF)(57.41±2.42对54.24±6.65;P < 0.001)恶化。
我们的研究结果表明,与RVP相比,CSP可能与HFpEF患者心脏功能改善和新发AHREs减少相关。然而,预计需要前瞻性随机试验来证实这些潜在益处。