Lee Cheol Whan, Lee Pil Hyung, Lee Seung-Whan, Serruys Patrick W
Division of Cardiology Heart Institute, Asan Medical Centre, University of Ulsan College of Medicine Seoul South Korea.
CORRIB Research Centre for Advanced Imaging and Core Lab University of Galway Galway Ireland.
Health Sci Rep. 2024 Dec 17;7(12):e70286. doi: 10.1002/hsr2.70286. eCollection 2024 Dec.
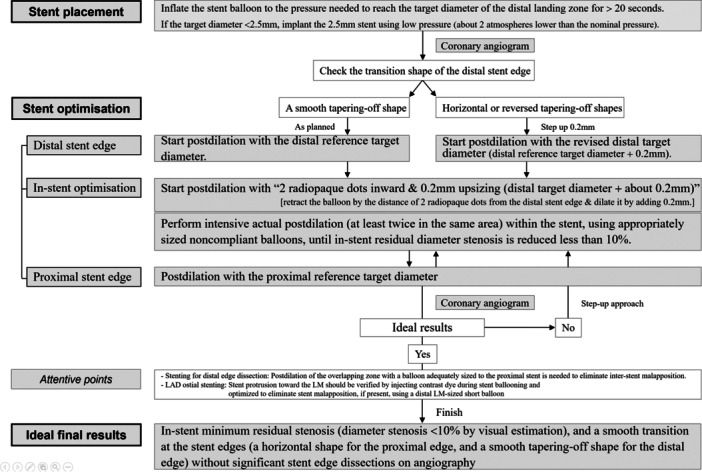
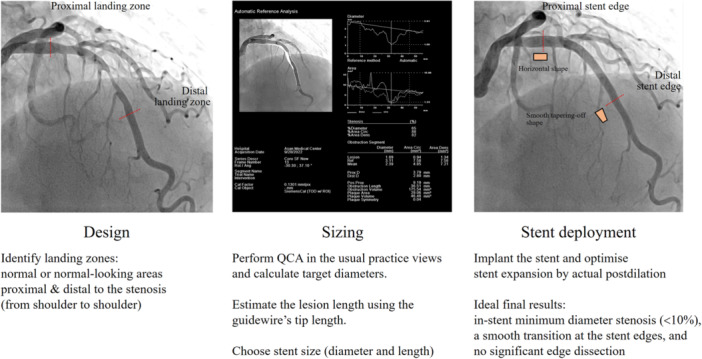
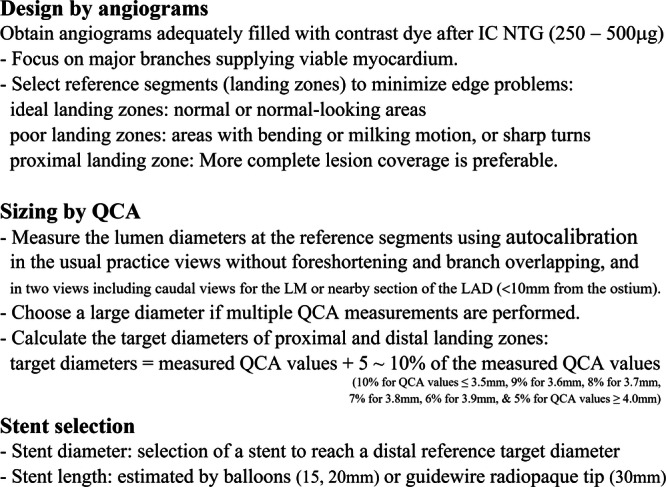
Percutaneous coronary intervention (PCI) using drug-eluting stents is an established strategy for the treatment of significant obstructive coronary artery disease. Evidence supports that intravascular imaging-guided PCI offers advantages over conventional angiography-guided PCI, though its use is limited, likely due to high costs. Angiography-guided PCI relies on visual estimation, leading to inter- and intra-observer variability and suboptimal outcomes. Quantitative coronary angiography (QCA) provides reliable information about vascular dimensions, overcoming these limitations. Poststenting postdilation with appropriately sized noncompliant balloons improves outcomes by increasing lumen area and reducing stent malapposition.
We investigated the procedural details of each modality used to guide PCI and assessed the utility of QCA-guided PCI with routine postdilation when intravascular imaging is unavailable.
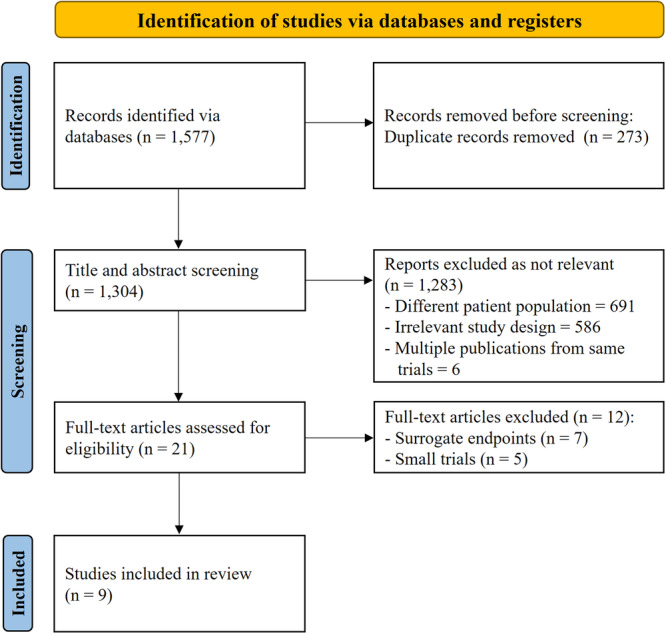
A systematic search was conducted from inception to May 31, 2024, identifying nine randomized controlled trials (with over 500 patients) that compared outcomes of PCI guided by intravascular imaging versus conventional angiography or QCA. The findings indicate that intravascular imaging guidance significantly improves clinical outcomes compared to angiography guidance. Notably, QCA-guided PCI with routine postdilation yielded outcomes comparable to those achieved with intravascular imaging-guided PCI.
QCA-guided PCI with routine postdilation may be a viable alternative for improving PCI outcomes, especially in settings where intravascular imaging is unavailable.
使用药物洗脱支架的经皮冠状动脉介入治疗(PCI)是治疗严重阻塞性冠状动脉疾病的既定策略。有证据支持血管内成像引导的PCI比传统血管造影引导的PCI更具优势,尽管其应用有限,可能是由于成本高昂。血管造影引导的PCI依赖于视觉估计,导致观察者间和观察者内的变异性以及不理想的结果。定量冠状动脉造影(QCA)提供了关于血管尺寸的可靠信息,克服了这些局限性。使用尺寸合适的非顺应性球囊进行支架置入后扩张可通过增加管腔面积和减少支架贴壁不良来改善结果。
我们研究了用于指导PCI的每种方式的操作细节,并评估了在无法进行血管内成像时,QCA引导并常规扩张的PCI的效用。
我们进行了一项从开始到2024年5月31日的系统检索,确定了9项随机对照试验(涉及500多名患者),这些试验比较了血管内成像引导与传统血管造影或QCA引导的PCI的结果。研究结果表明,与血管造影引导相比,血管内成像引导显著改善了临床结果。值得注意的是,QCA引导并常规扩张的PCI产生的结果与血管内成像引导的PCI相当。
QCA引导并常规扩张的PCI可能是改善PCI结果的可行替代方案,特别是在无法进行血管内成像的情况下。