Azaripour Adriano, Farina Vittorio Siro Leone, Esposito Marco, Buti Jacopo, Al-Nawas Bilal, Sagheb Keyvan
Department of Oral and Maxillofacial Surgery, University Medical Center, Johannes Gutenberg University, Augustusplatz 2, 55131, Mainz, Germany.
Department of Periodontology and Restorative Dentistry, University Medical Center, Johannes Gutenberg University, Mainz, Germany.
Int J Implant Dent. 2024 Dec 18;10(1):64. doi: 10.1186/s40729-024-00582-7.
To evaluate whether there are clinical benefits by preparing dental implant sites using piezosurgery instead of conventional rotary drills in healed bone crests and if initial crestal soft tissue thickness could have an impact on marginal bone loss.
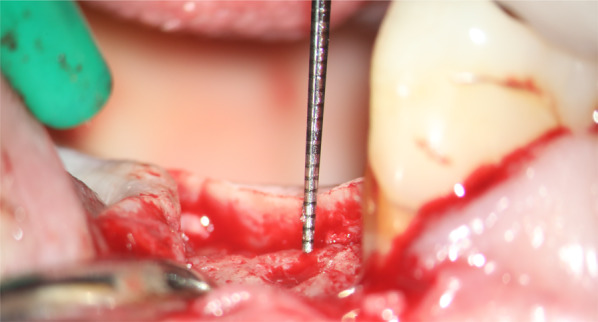
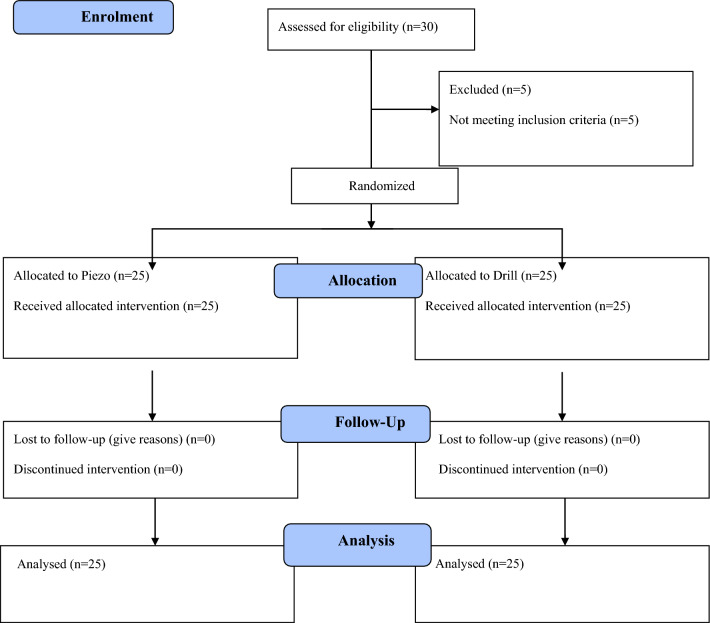
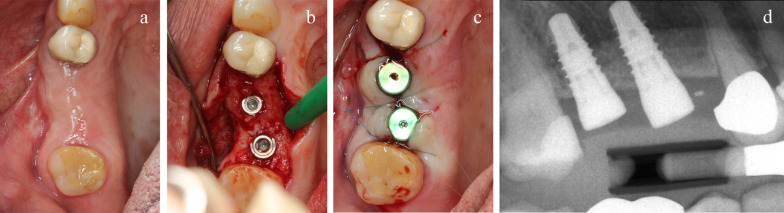
Twenty-five partially edentulous patients requiring two single implants in molar/premolar areas had each site randomly allocated to either piezosurgery or to conventional rotary drill preparation according to a split-mouth design. Definitive screw-retained metal-ceramic crowns were delivered after 6 months. All patients were followed to 5 years after placement. Outcome measures were: implant/crown failures, complications, peri-implant marginal bone level changes, resonance frequency analysis (RFA), and time required to complete site preparation, recorded, when possible, by blinded assessors.
No patients dropped-out and no implant failed. Five years after placement, there were no statistically significant differences for complications (only one complication in the piezo group: difference = 0.04; P = 1), for peri-implant bone loss (difference = -0.11 mm; 95% CI -0.24 to 0.01; P = 0.083), and for RFA changes (6 months) (difference = -0.35; 95% CI -1.95 to 1.25; P = 0.672 between groups). Significantly more time was needed to prepare implant sites with piezosurgery (difference = 236.8 s; 95% CI -286.12 to -187.48; P < 0.0001). Initial soft tissue thickness had no effect on peri-implant bone loss (estimate = 0.05; 95% CI -0.03; 0.12; P = 0.239).
No clinically appreciable differences were noticed when placing implants using piezosurgery or conventional instrumentation with rotary drill, however, the preparation with rotary drills was on average 4 min faster. No effect of initial crestal soft tissue thickness was observed on peri-implant bone loss.
评估在愈合的牙槽嵴中使用超声骨刀而非传统旋转钻制备牙种植位点是否具有临床益处,以及初始牙槽嵴软组织厚度是否会对边缘骨吸收产生影响。
25例需要在磨牙/前磨牙区域植入两颗单颗种植体的部分牙列缺损患者,根据分口设计将每个位点随机分配至超声骨刀组或传统旋转钻制备组。6个月后安装最终的螺丝固位金属烤瓷冠。所有患者在种植体植入后随访5年。观察指标包括:种植体/牙冠失败情况、并发症、种植体周围边缘骨水平变化、共振频率分析(RFA)以及完成位点制备所需的时间(如有可能,由盲法评估者记录)。
无患者退出研究,也没有种植体失败。种植体植入5年后,两组在并发症(超声骨刀组仅1例并发症:差异 = 0.04;P = 1)、种植体周围骨吸收(差异 = -0.11 mm;95%可信区间 -0.24至0.01;P = 0.083)以及RFA变化(6个月时)(差异 = -0.35;95%可信区间 -1.95至1.25;组间P = 0.672)方面均无统计学显著差异。使用超声骨刀制备种植位点需要更多时间(差异 = 236.8秒;95%可信区间 -286.12至 -187.48;P < 0.0001)。初始软组织厚度对种植体周围骨吸收没有影响(估计值 = 0.05;95%可信区间 -0.03;0.12;P = 0.239)。
使用超声骨刀或传统旋转钻器械植入种植体时,未观察到临床上明显的差异,然而,使用旋转钻制备平均快4分钟。未观察到初始牙槽嵴软组织厚度对种植体周围骨吸收有影响。