Barnicle Alan, Ray-Coquard Isabelle, Rouleau Etienne, Cadoo Karen, Simpkins Fiona, Aghajanian Carol, Leary Alexandra, Poveda Andrés, Lheureux Stephanie, Pujade-Lauraine Eric, You Benoit, Ledermann Jonathan, Matulonis Ursula, Gourley Charlie, Timms Kirsten M, Lai Zhongwu, Hodgson Darren R, Elks Cathy E, Dearden Simon, Egile Coumaran, Lao-Sirieix Pierre, Harrington Elizabeth A, Brown Jessica S
Translational Medicine, Oncology R&D, AstraZeneca, Cambridge Biomedical Campus, 1 Francis Crick Avenue, Cambridge, CB2 0AA, UK.
Medical Oncology Department, Centre Léon Bérard and University Claude Bernard Lyon, and Groupe d'Investigateurs Nationaux pour l'Etude des Cancers Ovariens (GINECO), Lyon, France.
Genome Med. 2024 Dec 18;16(1):145. doi: 10.1186/s13073-024-01413-5.
The introduction of poly(ADP-ribose) polymerase (PARP) inhibitors represented a paradigm shift in the treatment of ovarian cancer. Genomic data from patients with high-grade ovarian cancer in six phase II/III trials involving the PARP inhibitor olaparib were analyzed to better understand patterns and potential causes of genomic instability.
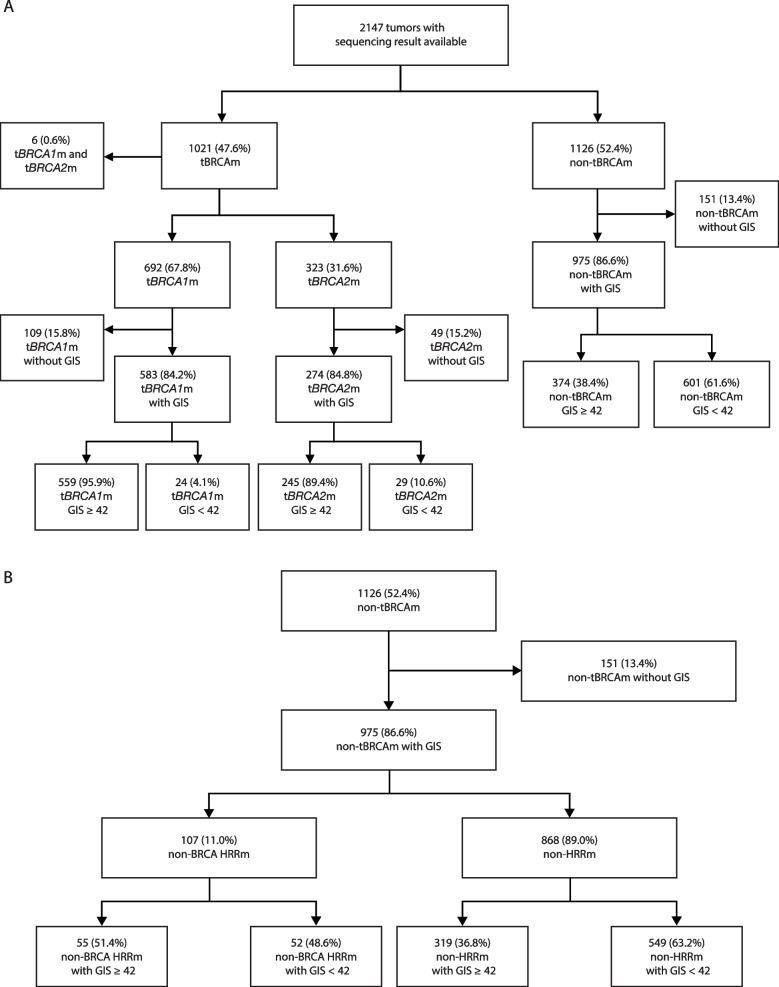
Homologous recombination deficiency (HRD) was assessed in 2147 tumor samples from SOLO1, PAOLA-1, Study 19, SOLO2, OPINION, and LIGHT using next-generation sequencing technology. Genomic instability scores (GIS) were assessed in BRCA1 and/or BRCA2 (BRCA)-mutated (BRCAm), non-BRCA homologous recombination repair-mutated (non-BRCA HRRm), and non-HRRm tumors.
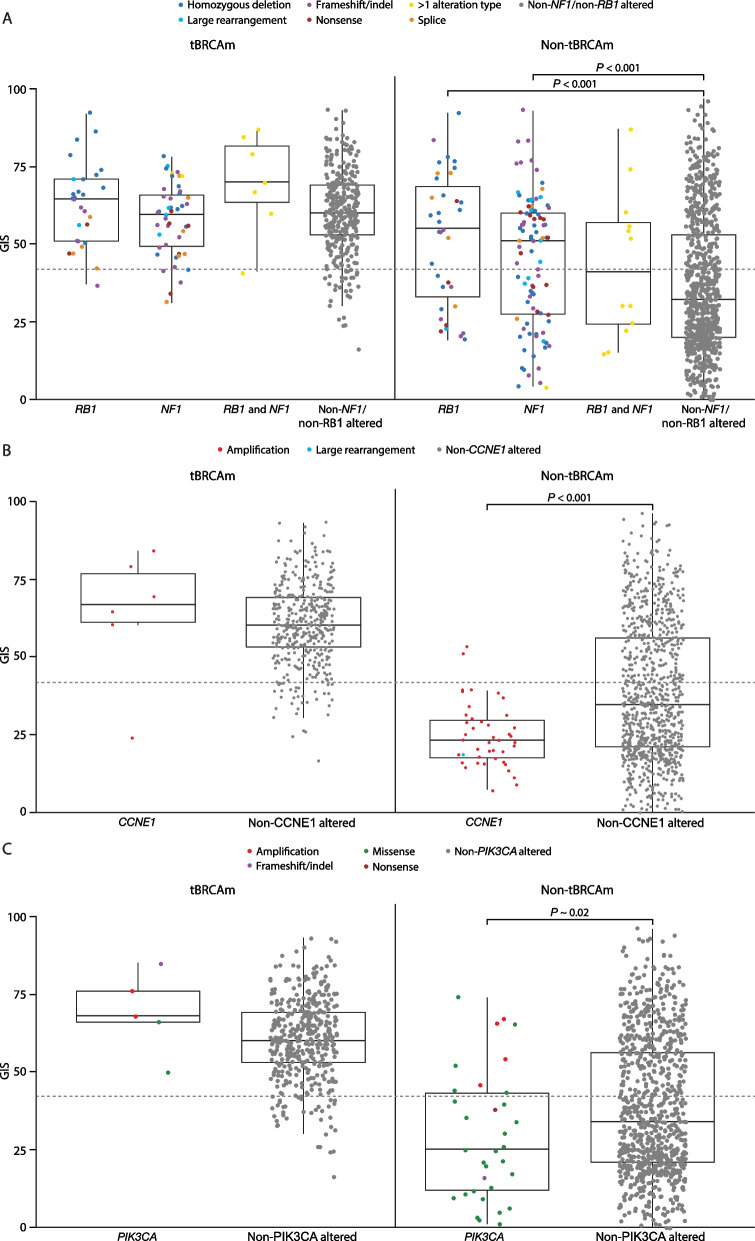
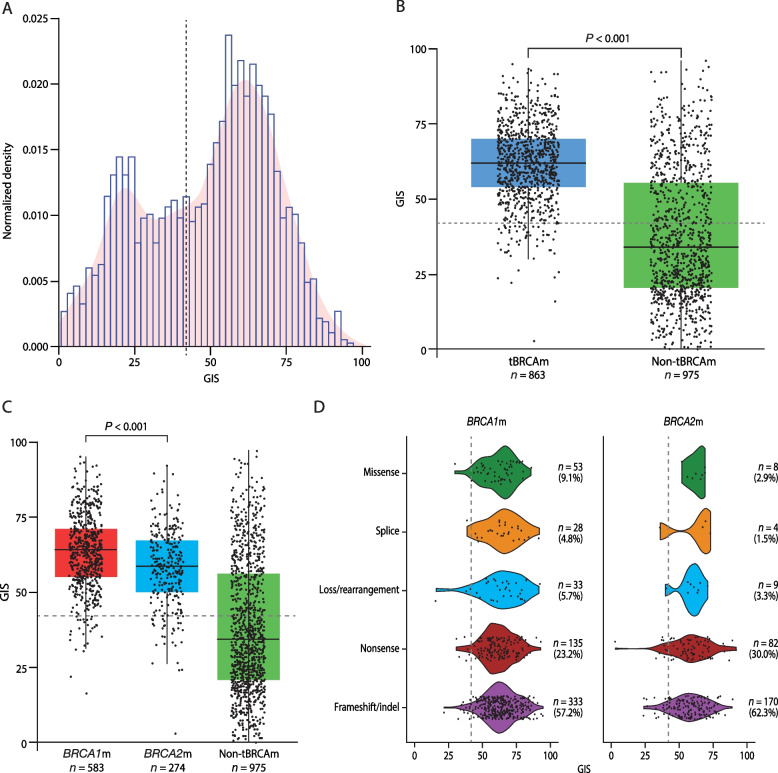
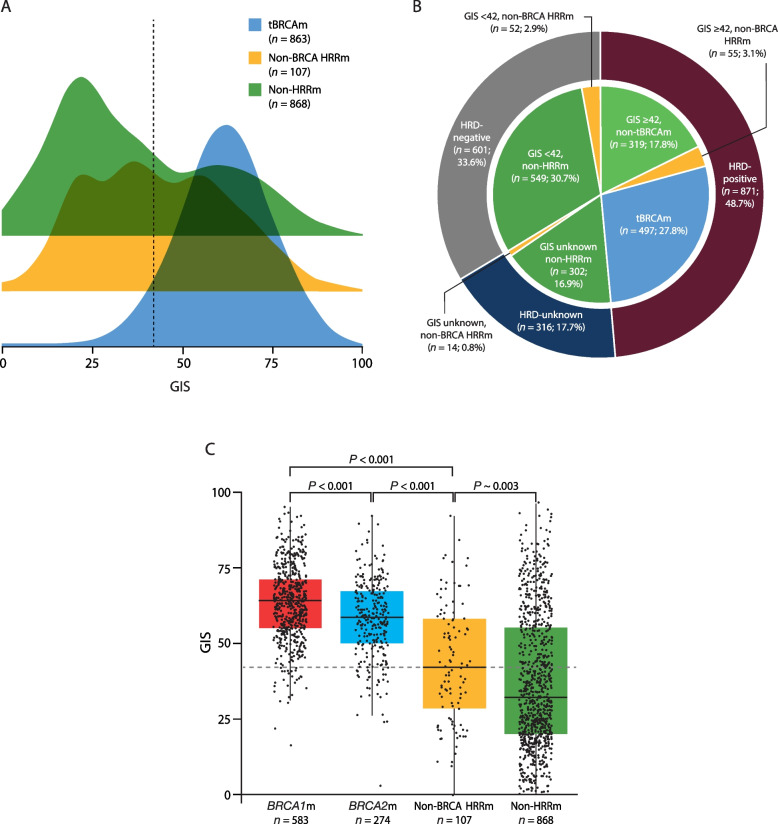
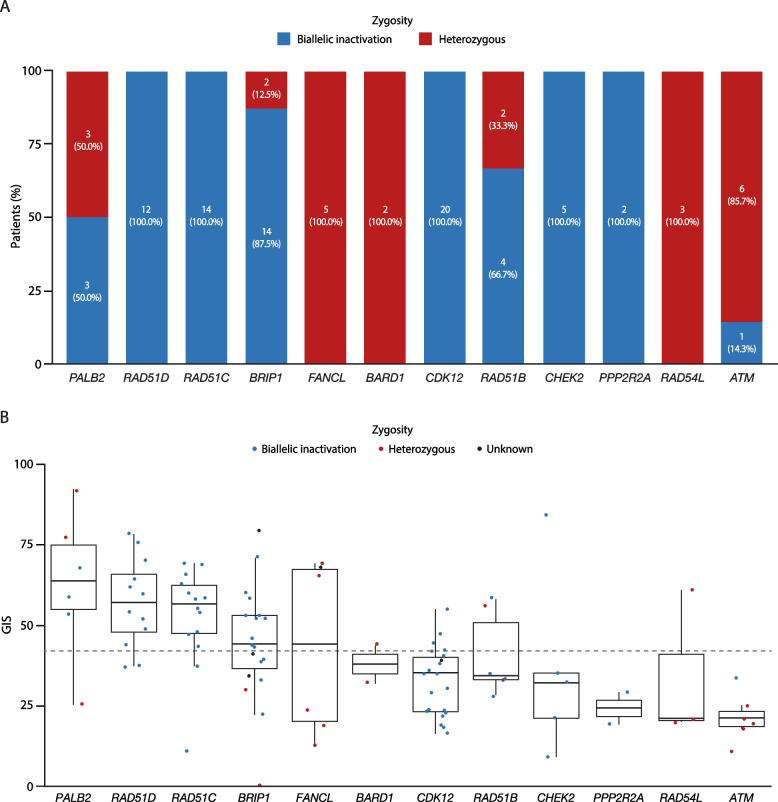
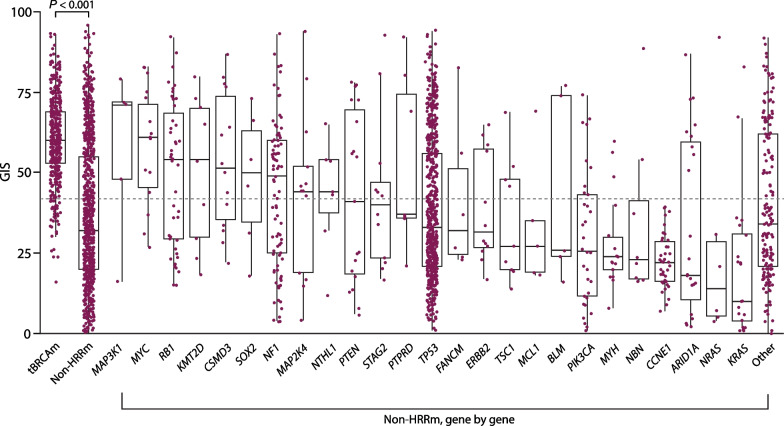
BRCAm was identified in 1021/2147 (47.6%) tumors. BRCAm tumors had significantly higher GIS than non-BRCAm tumors (P < 0.001) and high biallelic loss (815/838; 97.3%) regardless of germline (658/672; 97.9%) or somatic (101/108; 93.5%) BRCAm status. In non-BRCA HRRm tumors (n = 121) a similar proportion were HRD-positive (GIS ≥ 42: 55/121; 45.5%) relative to HRD-negative (GIS < 42: 52/121; 43.0%). GIS was highly variable in non-BRCA HRRm (median 42 [interquartile range (IQR) 29-58]) and non-HRRm (n = 1005; median 32 [IQR 20-55]) tumors. Gene mutations with high GIS included HRR genes BRIP1 (median 46 [IQR 41-58]), RAD51C (median 58 [IQR 48-66]), RAD51D (median 62 [IQR 54-69]), and PALB2 (median 64 [IQR 58-74]), and non-HRR genes NF1 (median 49 [IQR 25-60]) and RB1 (median 55 [IQR 30-71]). CCNE1-amplified and PIK3CA-mutated tumors had low GIS (CCNE1-amplified: median 24 [IQR 18-29]; PIK3CA-mutated: median 32 [IQR 14-52]) and were predominantly non-BRCAm.
These analyses provide valuable insight into patterns of genomic instability and potential drivers of HRD, besides BRCAm, in ovarian cancer and will help guide future research into the potential clinical effectiveness of anti-cancer treatments in ovarian cancer, including PARP inhibitors as well as other precision oncology agents.
The SOLO1 trial was registered at ClinicalTrials.gov (NCT01844986) on April 30, 2013; the PAOLA-1 trial was registered at ClinicalTrials.gov (NCT02477644) on June 18, 2015 (retrospectively registered); Study 19 was registered at ClinicalTrials.gov (NCT00753545) on September 12, 2008 (retrospectively registered); the SOLO2 trial was registered at ClinicalTrials.gov (NCT01874353) on June 7, 2013; the OPINION trial was registered at ClinicalTrials.gov (NCT03402841) on January 3, 2018; the LIGHT trial was registered at ClinicalTrials.gov (NCT02983799) on November 4, 2016.
聚(ADP - 核糖)聚合酶(PARP)抑制剂的引入代表了卵巢癌治疗的范式转变。对六项涉及PARP抑制剂奥拉帕利的II/III期试验中高级别卵巢癌患者的基因组数据进行分析,以更好地了解基因组不稳定的模式和潜在原因。
使用下一代测序技术对来自SOLO1、PAOLA - 1、研究19、SOLO2、OPINION和LIGHT的2147个肿瘤样本进行同源重组缺陷(HRD)评估。在BRCA1和/或BRCA2(BRCA)突变(BRCAm)、非BRCA同源重组修复突变(非BRCA HRRm)和非HRRm肿瘤中评估基因组不稳定评分(GIS)。
在1021/2147(47.6%)的肿瘤中鉴定出BRCAm。BRCAm肿瘤的GIS显著高于非BRCAm肿瘤(P < 0.001),且无论种系(658/672;97.9%)或体细胞(101/108;93.5%)BRCAm状态如何,均有高双等位基因缺失(815/838;97.3%)。在非BRCA HRRm肿瘤(n = 121)中,HRD阳性(GIS≥42:55/121;45.5%)的比例与HRD阴性(GIS < 42:52/121;43.0%)相似。GIS在非BRCA HRRm(中位数42 [四分位间距(IQR)29 - 58])和非HRRm(n = 1005;中位数32 [IQR 20 - 55])肿瘤中高度可变。GIS高的基因突变包括HRR基因BRIP1(中位数46 [IQR 41 - 58])、RAD51C(中位数58 [IQR 48 - 66])、RAD51D(中位数62 [IQR 54 - 69])和PALB2(中位数64 [IQR 58 - 74]),以及非HRR基因NF1(中位数49 [IQR 25 - 60])和RB1(中位数55 [IQR 30 - 71])。CCNE1扩增和PIK3CA突变的肿瘤GIS较低(CCNE1扩增:中位数24 [IQR 18 - 29];PIK3CA突变:中位数32 [IQR 14 - 52]),且主要为非BRCAm。
这些分析为卵巢癌中除BRCAm之外的基因组不稳定模式和HRD的潜在驱动因素提供了有价值的见解,并将有助于指导未来关于卵巢癌抗癌治疗(包括PARP抑制剂以及其他精准肿瘤学药物)潜在临床疗效的研究。
SOLO1试验于2013年4月30日在ClinicalTrials.gov注册(NCT01844986);PAOLA - 1试验于2015年6月18日在ClinicalTrials.gov注册(NCT02477644)(追溯注册);研究19于2008年9月12日在ClinicalTrials.gov注册(NCT00753545)(追溯注册);SOLO2试验于2013年6月7日在ClinicalTrials.gov注册(NCT01874353);OPINION试验于2018年1月3日在ClinicalTrials.gov注册(NCT03402841);LIGHT试验于2016年11月4日在ClinicalTrials.gov注册(NCT02983799)。