Arns Beatriz, Kalil Andre C, Sorio Guilherme G L, Boschi Emerson, Antonio Ana Carolina Peçanha, Antonio Juliana Peçanha, Birriel Daniella Cunha, Lanziotti Daniel Haase, da Cunha Abbott Frederico, Rocha Glecia Carla, de Fátima Fernandes Vanildes, de Souza Dantas Vicente Cés, da Silva Medeiros Graciele Fátima, de França Diniz Rocha Verônica, Pereira Francielle Constantino, Gobatto André Luiz Nunes, Lima Valéria Paes, Lacerda Fábio Holanda, de Maio Carrilho Cláudia Maria Dantas, de Oliveira Cardozo Kairo Daniel Nunes, Irineu Vivian Menezes, Kurtz Pedro, Horvath Jaqueline Driemeyer Correia, Sesin Guilhermo Prates, Agani Crepin Aziz Jose Oluwafoumi, Dos Santos Tiago Marcon, Brochier Liliane Spencer Bittencourt, da Rosa Bruna Silveira, Tomazini Bruno Martins, Besen Bruno Adler Maccagnan Pinheiro, Pereira Adriano Jose, Veiga Viviane Cordeiro, Nascimento Giovana Marssola, Zavascki Alexandre P
Infectious Diseases and Infection Control Service, Hospital Moinhos de Vento, 910 Ramiro Barcelos St, Porto Alegre, RS, 90035-000, Brazil.
Responsabilidade Social - PROADI, Hospital Moinhos de Vento, Porto Alegre, RS, Brazil.
Crit Care. 2024 Dec 18;28(1):412. doi: 10.1186/s13054-024-05178-6.
Shorter courses of antimicrobial therapy have been shown to be non-inferior to longer durations for the management of several infections. However, data on critically ill patients with severe infections by multidrug-resistant Gram-negative bacteria (MDR-GNB) are scarce. In the duratiOn of theraPy in severe infecTIons by MultIdrug-reSistant gram-nEgative bacteria (OPTIMISE) trial, we assessed the non-inferiority of 7-day versus 14-day antimicrobial therapy for patients with intensive care unit (ICU)-acquired severe infections by MDR-GNB.
This was a randomised multicenter, open-label, parallel controlled, non-inferiority trial. Adult patients with severe infections by MDR-GNB initiated ≥ 48 h of ICU admission were eligible if they were hemodynamically stable and without fever > 48 h on the 7th day of appropriate antimicrobial therapy. Patients were 1:1 randomised to discontinue antimicrobial therapy on the 7th (± 1) day or to continue for a total of 14 (± 1) days. The primary outcome was clinical failure, defined as death or relapse of infection within 28 days of randomisation. An upper edge of the two-tailed 95% confidence interval (CI) of the delta between the clinical failure rate in the 7- and the 14-day lower than 10% in both intention-to-treat (ITT) and per protocol (PP) analyses was set as the non-inferiority criteria.
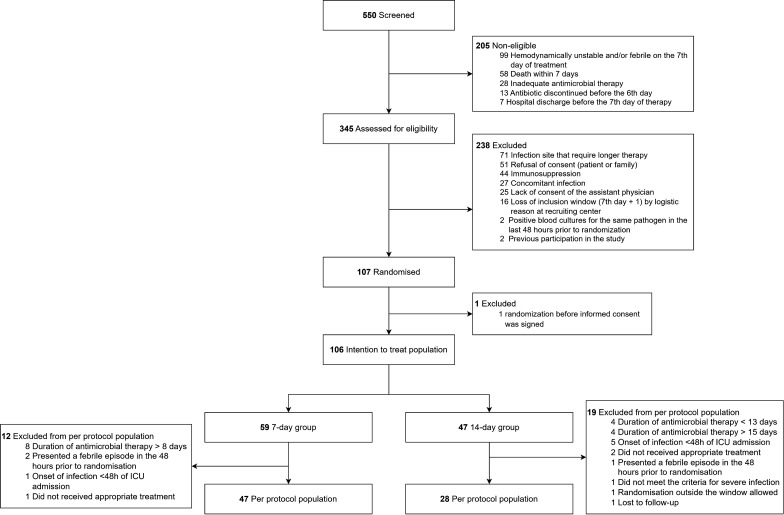
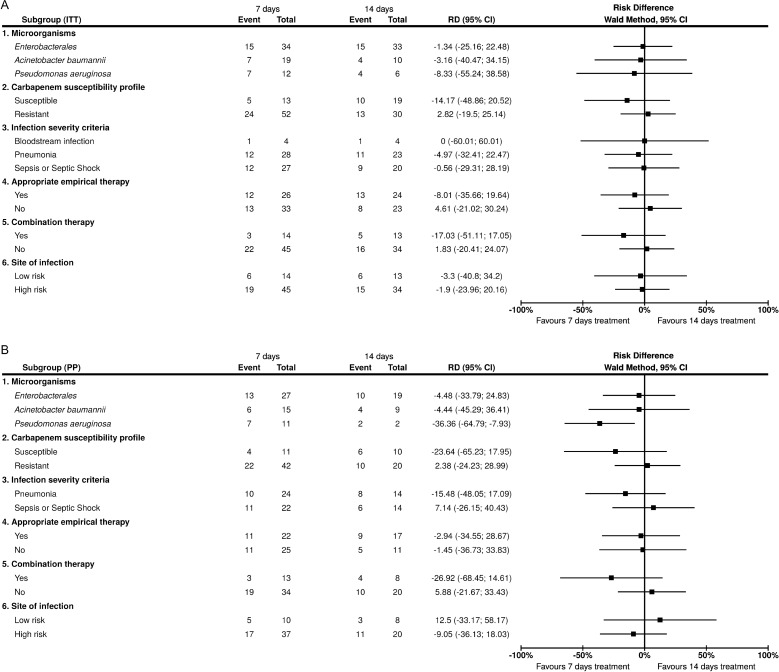
A total of 106 patients composed the ITT population: 59 and 47 allocated to 7- and 14-day groups, respectively. The PP population included 75 patients: 47 and 28 in the 7- and 14-day groups, respectively. Clinical failure occurred in 42.4% and 44.7% of the ITT population in 7- and 14-day groups, respectively, (risk difference (RD) - 2.3, 95%CI - 21.3 to 16.7), and in 46.8% and 50.0% of the PP population in 7- and 14-day groups, respectively (RD - 3.2, 95%CI - 26.6 to 20.2). Most infections were of the respiratory tract (73/68.9%) and caused by carbapenem-resistant Enterobacterales (42/39.6%). The study was interrupted before reaching planned sample size due to low recruitment rate.
The OPTIMISE trial could not determine the non-inferiority of 7-day compared to 14-day therapy for severe infections caused by MDR-GNB due to early termination related to the low recruitment rate.
NCT05210387 on January 13, 2022.
对于多种感染的治疗,较短疗程的抗菌治疗已被证明不劣于较长疗程。然而,关于耐多药革兰氏阴性菌(MDR - GNB)引起的重症感染患者的数据却很稀少。在耐多药革兰氏阴性菌引起的严重感染治疗疗程(OPTIMISE)试验中,我们评估了7天与14天抗菌治疗对重症监护病房(ICU)获得性耐多药革兰氏阴性菌严重感染患者的非劣效性。
这是一项随机、多中心、开放标签、平行对照的非劣效性试验。因耐多药革兰氏阴性菌导致严重感染的成年患者,在入住ICU≥48小时后,如果血流动力学稳定且在适当抗菌治疗第7天时无发热>48小时,则符合入选标准。患者按1:1随机分为在第7(±1)天停止抗菌治疗组或总共持续14(±1)天治疗组。主要结局为临床失败,定义为随机分组后28天内死亡或感染复发。在意向性分析(ITT)和符合方案分析(PP)中,7天和14天临床失败率差值的双侧95%置信区间(CI)上限低于10%被设定为非劣效性标准。
共有106例患者组成ITT人群:分别有59例和47例被分配到7天和14天治疗组。PP人群包括75例患者:7天和14天治疗组分别有47例和28例。7天和14天治疗组的ITT人群中临床失败发生率分别为42.4%和44.7%(风险差(RD)-2.3,95%CI -21.3至16.7),PP人群中分别为46.8%和50.0%(RD -3.2,95%CI -26.6至20.2)。大多数感染为呼吸道感染(73/68.9%),由耐碳青霉烯类肠杆菌科细菌引起(42/39.6%)。由于招募率低,该研究在达到计划样本量之前就中断了。
由于招募率低导致早期终止,OPTIMISE试验无法确定7天治疗与14天治疗相比对耐多药革兰氏阴性菌引起的严重感染的非劣效性。
2022年1月13日NCT05210387 。