Bierer Joel, Stanzel Roger, Henderson Mark, Sapp John, Andreou Pantelis, Marshall Jean S, Horne David
Division of Cardiac Surgery, IWK Children's Heart CentreDivision of Cardiac Surgery, Dalhousie University, Halifax, Canada.
Department of Clinical Perfusion, Nova Scotia Health Authority, Halifax, Canada.
Eur J Med Res. 2024 Dec 19;29(1):601. doi: 10.1186/s40001-024-02156-0.
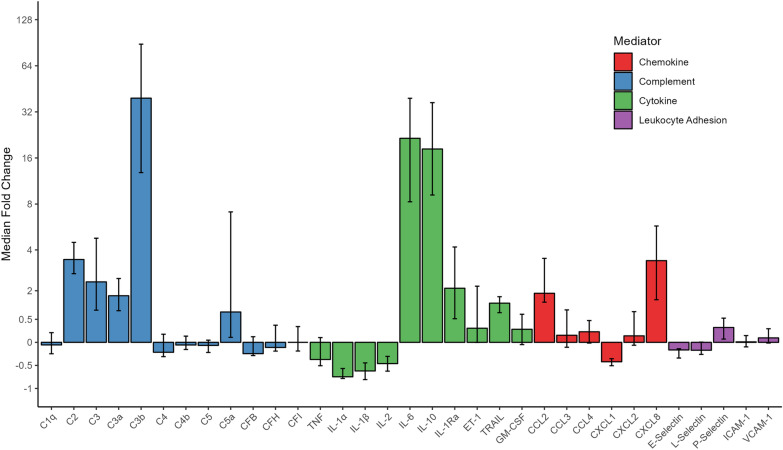
Cardiopulmonary bypass (CPB) causes systemic inflammation during pediatric cardiac surgery, which can contribute to post-operative organ dysfunction and prolonged recovery. This study aims to identify key inflammatory mediators related to this clinically significant immunologic response.
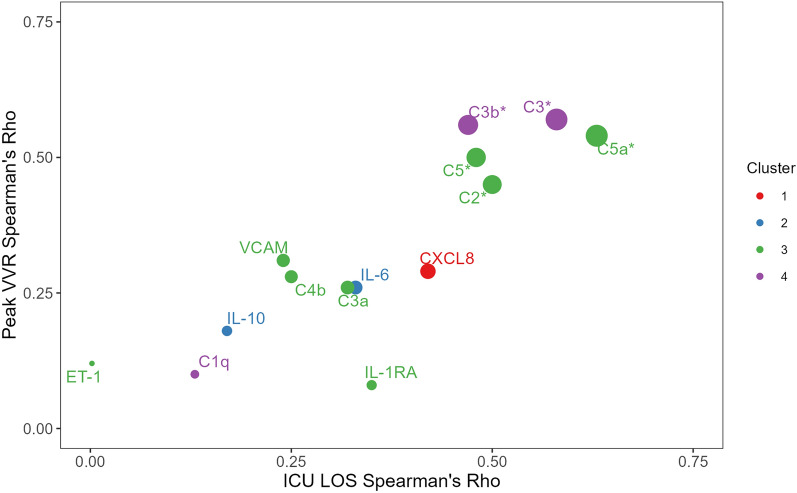
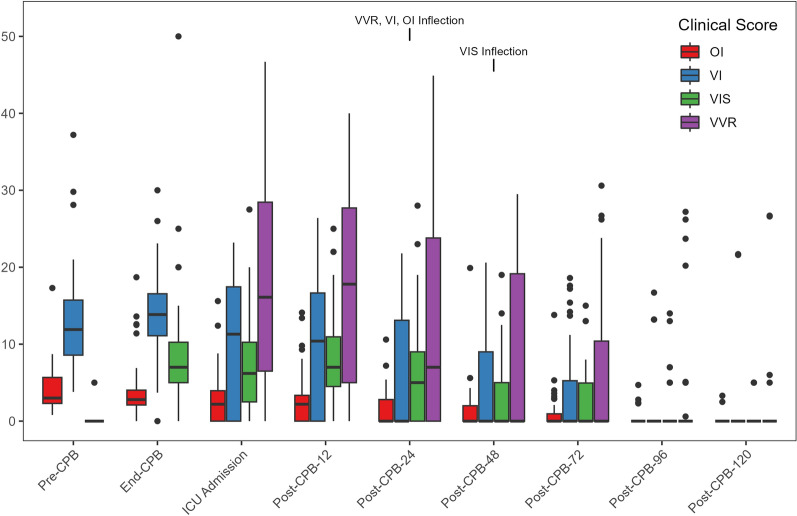
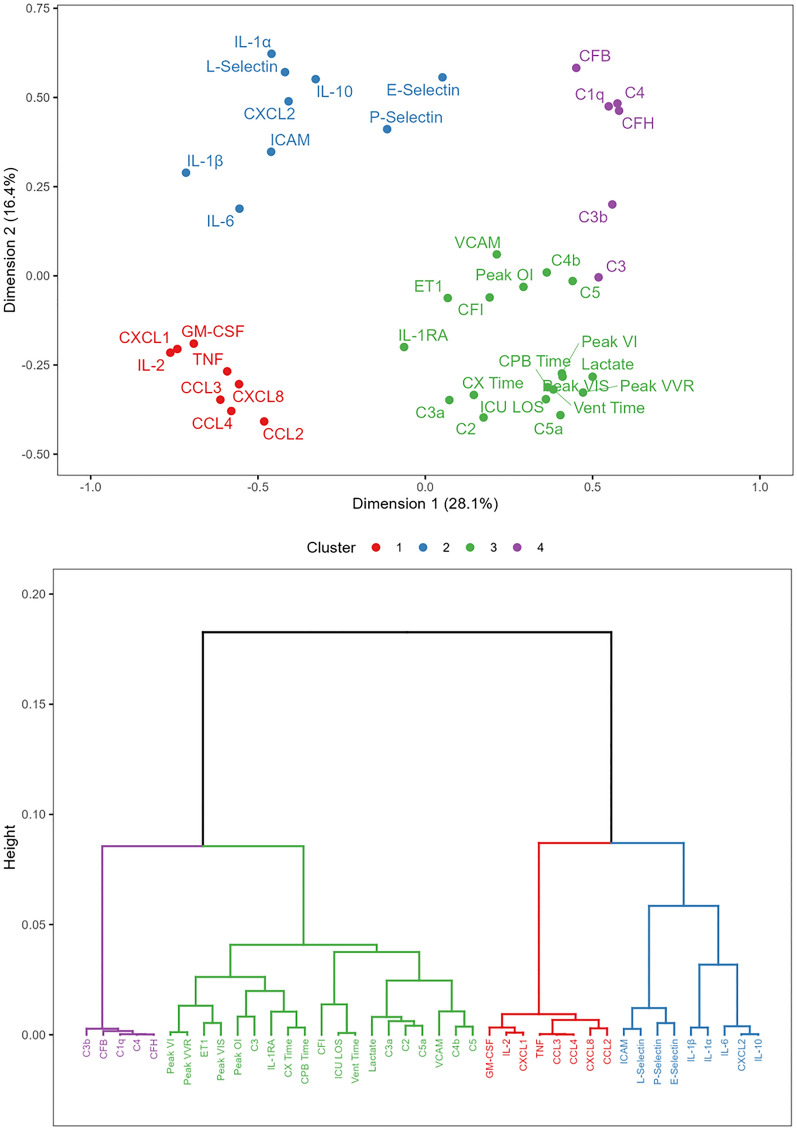
Pediatric patients were enrolled in a single-arm prospective clinical study (NCT05154864) and received standard cardiac operation, CPB and subzero-balance ultrafiltration. Arterial samples were taken before CPB initiation and immediately after weaning, and concentrations of 33 inflammatory mediators were assayed. A principal component analysis with hierarchical clustering (PCA-HCPC) included inflammatory mediator concentrations measured at the end of CPB, validated peak post-operative clinical scores, ventilation time and intensive care length of stay. Mahalanobis distance assessed statistical differences between clusters. Spearman's correlation described the linear relationship between mediator concentrations at the end of CPB and intensive care length of stay. Results are median (IQR).
Forty consecutive patients were enrolled; the majority were male (58%), age of 7.3 (1.7-39.0) months and weight of 6.7 (4.6-14.9) kg. The PCA-HCPC revealed activated complement factors along with all peak clinical scores and prolonged intensive care requirements in the same cluster. Cytokine, chemokine, and leukocyte adhesion molecule concentrations were found in two other distinct clusters (Mahalanobis distance = 16.5; p = 0.004 and Mahalanobis distance = 17.4; p = 5.8 × 10). Mediator concentrations of C2 (Rho = 0.50; p = 0.001), C3 (Rho = 0.58; p = 1.1 × 10), C3b (Rho = 0.47; p = 0.002), C5 (Rho = 0.48; p = 0.002) and C5a (Rho = 0.63; 1.7 × 10) showed linear correlations with intensive care unit length of stay.
Activated complement factors, but not pro-inflammatory cytokines or chemokines, were most related to cardiopulmonary dysfunction and prolonged recovery in this novel analysis. Investigation of therapies that inhibit complement to dampen CPB-associated inflammation and enhance recovery after pediatric cardiac surgery is warranted. Trial Registration ClinicalTrials.gov, NCT05154864.
体外循环(CPB)在小儿心脏手术期间会引发全身炎症反应,这可能导致术后器官功能障碍和恢复时间延长。本研究旨在确定与这种具有临床意义的免疫反应相关的关键炎症介质。
小儿患者纳入一项单臂前瞻性临床研究(NCT05154864),接受标准心脏手术、CPB和零平衡超滤。在CPB开始前和脱机后立即采集动脉样本,检测33种炎症介质的浓度。主成分分析与层次聚类(PCA-HCPC)纳入了CPB结束时测量的炎症介质浓度、验证后的术后临床评分峰值、通气时间和重症监护住院时间。马氏距离评估各聚类之间的统计学差异。Spearman相关性描述了CPB结束时介质浓度与重症监护住院时间之间的线性关系。结果为中位数(IQR)。
连续纳入40例患者;大多数为男性(58%),年龄7.3(1.7 - 39.0)个月,体重6.7(4.6 - 14.9)kg。PCA-HCPC显示活化补体因子与所有临床评分峰值以及同一聚类中延长的重症监护需求相关。细胞因子、趋化因子和白细胞黏附分子浓度出现在另外两个不同聚类中(马氏距离 = 16.5;p = 0.004和马氏距离 = 17.4;p = 5.8×10)。C2(Rho = 0.50;p = 0.001)、C3(Rho = 0.58;p = 1.1×10)、C3b(Rho = 0.47;p = 0.002)、C5(Rho = 0.48;p = 0.002)和C5a(Rho = 0.63;1.7×10)的介质浓度与重症监护病房住院时间呈线性相关。
在这项新分析中,活化补体因子而非促炎细胞因子或趋化因子与心肺功能障碍和恢复时间延长最为相关。有必要研究抑制补体以减轻CPB相关炎症并促进小儿心脏手术后恢复的治疗方法。试验注册ClinicalTrials.gov,NCT05154864。