Matikas Alexios, Papakonstantinou Andri, Loibl Sibylle, Steger Günther G, Untch Michael, Johansson Hemming, Tsiknakis Nikos, Hellström Mats, Greil Richard, Möbus Volker, Gnant Michael, Bergh Jonas, Foukakis Theodoros
Karolinska Institutet, Oncology/Pathology Department, Stockholm, Sweden.
Breast Center, Karolinska Comprehensive Cancer Center, Stockholm, Sweden.
Lancet Reg Health Eur. 2024 Dec 3;49:101162. doi: 10.1016/j.lanepe.2024.101162. eCollection 2025 Feb.
It is unclear whether some patients with high-risk breast cancer do not warrant adjuvant dose-dense chemotherapy due to small expected absolute benefit.
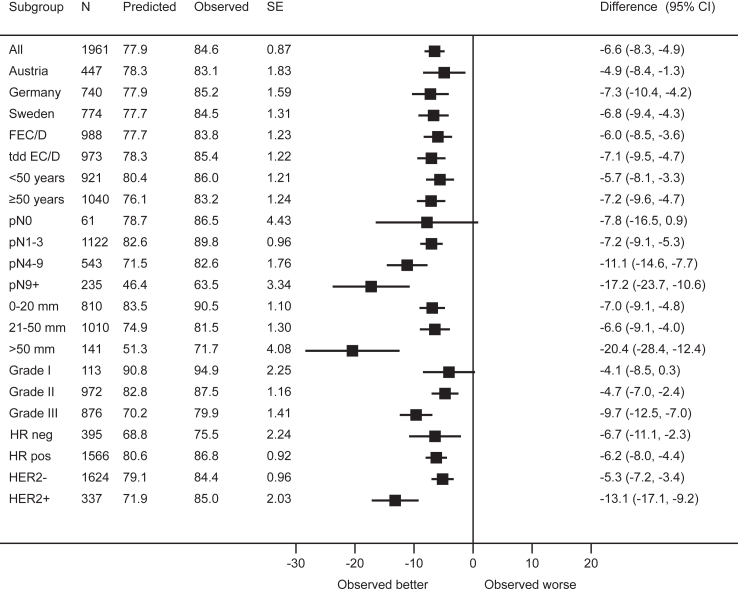
The phase 3 PANTHER trial (NCT00798070) compared adjuvant sequential epirubicin/cyclophosphamide (EC) and docetaxel (D) administered in either tailored dose-dense (tDD EC/D) or standard interval schedule (FEC/D) to patients with high-risk resected early breast cancer (n = 2003). We compared outcomes across key subgroups of interest, evaluated the performance of the online prognostication and treatment benefit estimation tool PREDICT and conducted a subpopulation treatment effect pattern plot (STEPP) analysis. Primary endpoint was breast cancer recurrence free survival (BCRFS).
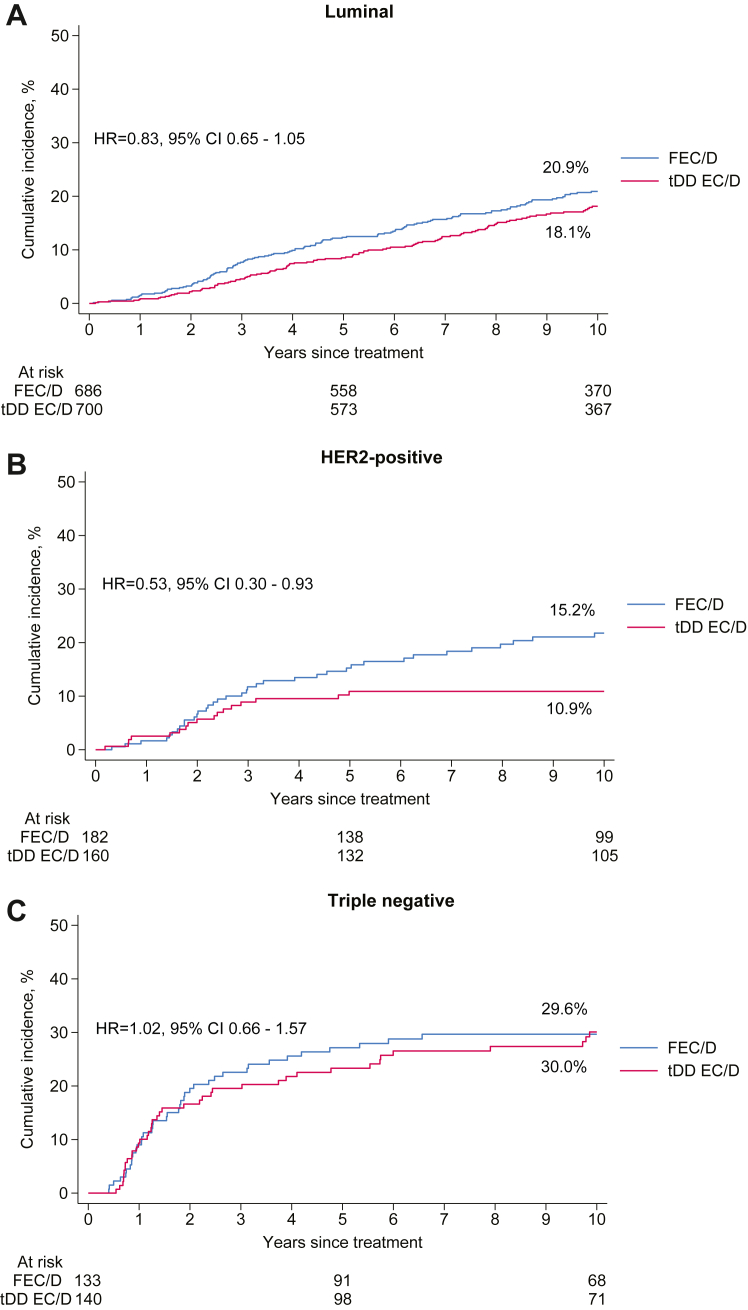
Median follow-up was 10.3 years. Treatment with tDD EC/D improved 10-year BCRFS across all subgroups including according to menopausal status, with an absolute benefit of 2% or more, as well as in luminal (Hazard Ratio [HR] = 0.83, 95% Confidence Interval [CI] 0.65-1.05) and Human Epidermal Growth Factor Receptor 2 (HER2) positive (HR = 0.53, 95% CI 0.30-0.93), but not triple negative breast cancer patients (HR = 1.02, 95% CI 0.66-1.57). PREDICT underestimated overall survival in the entire population and across all subgroups. In STEPP analysis, absolute benefit from tDD EC/D in BCRFS was stable across risk-defined subpopulations, from 3.8% in the lowest risk patients to 3.6% in the highest risk ones. There was no differential treatment effect over time.
We could not reliably identify any subgroup not benefiting from dose-dense treatment, which should be considered for patients with primary resected high-risk breast cancer.
Cancerfonden, Bröstcancerförbundet, Radiumhemmets Forskningsfonder, Amgen, Roche, sanofi-aventis.
目前尚不清楚部分高危乳腺癌患者是否因预期的绝对获益较小而不值得接受辅助剂量密集化疗。
3期PANTHER试验(NCT00798070)将辅助序贯表柔比星/环磷酰胺(EC)和多西他赛(D),以定制剂量密集(tDD EC/D)或标准间隔方案(FEC/D)给药,用于治疗高危早期乳腺癌切除患者(n = 2003)。我们比较了各关键亚组的结局,评估了在线预后和治疗获益评估工具PREDICT的性能,并进行了亚组治疗效应模式图(STEPP)分析。主要终点是无乳腺癌复发生存期(BCRFS)。
中位随访时间为10.3年。tDD EC/D治疗在所有亚组中均改善了10年BCRFS,包括根据绝经状态划分的亚组,绝对获益为2%或更多,在管腔型(风险比[HR]=0.83,95%置信区间[CI]0.65 - 1.05)和人表皮生长因子受体2(HER2)阳性(HR = 0.53,95% CI 0.30 - 0.93)患者中也是如此,但三阴性乳腺癌患者除外(HR = 1.02,95% CI 0.66 - 1.57)。PREDICT低估了总体人群和所有亚组的总生存期。在STEPP分析中,tDD EC/D在BCRFS方面的绝对获益在风险定义的亚组中保持稳定,从最低风险患者的3.8%到最高风险患者的3.6%。随着时间推移没有差异治疗效应。
我们无法可靠地识别出任何未从剂量密集治疗中获益的亚组,对于原发性高危乳腺癌切除患者应考虑采用该治疗方法。
瑞典癌症基金会、瑞典乳腺癌协会、镭医院研究基金会、安进公司、罗氏公司、赛诺菲 - 安万特公司。