Camarda F, Mastrantoni L, Parrillo C, Minucci A, Persiani F, Giannarelli D, Pasciuto T, Giacomini F, De Paolis E, Manfredelli M, Marchetti C, Zannoni G F, Fagotti A, Scambia G, Nero C
Unit of Oncological Gynecology, Women's Children's and Public Health Department, Fondazione Policlinico Universitario Agostino Gemelli, IRCCS, Rome, Italy. Electronic address: https://twitter.com/FlorianaCamarda.
Medical Oncology, Università Cattolica del Sacro Cuore, Rome, Italy.
ESMO Open. 2025 Jan;10(1):104090. doi: 10.1016/j.esmoop.2024.104090. Epub 2024 Dec 19.
According to the European Society for Clinical Oncology (ESMO) guidelines, the therapeutic algorithm for early-stage epithelial ovarian carcinoma (EOC) is primarily based on grading and histotype. Adjuvant chemotherapy is usually recommended for high-grade tumors and for the International Federation of Gynecology and Obstetrics (FIGO) stage IB-IC; however, overtreatment remains a concern. Conversely, patients truly at higher risk of recurrence currently lack access to additional therapeutic strategies.
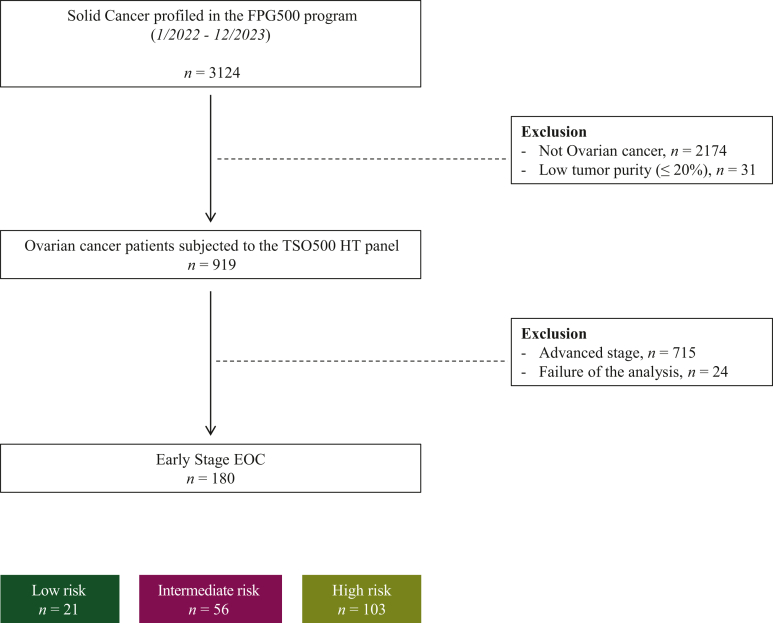
This study presents a descriptive analysis of early-stage EOC patients who were prospectively sequenced and stratified into high-, intermediate-, and low-risk groups based on clinicopathological features. Oncogenic alterations were identified using OncoKB and classified according to the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT) Tier I-III. The prevalence of molecular findings was first reported for each risk subgroup, followed by an analysis on the cohort of patients who experienced relapse.
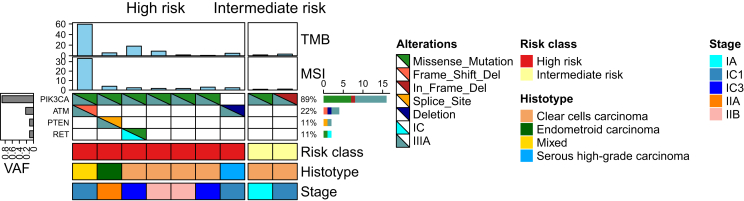
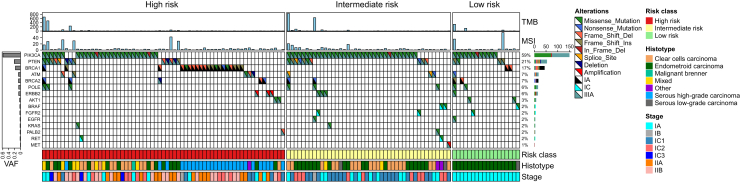
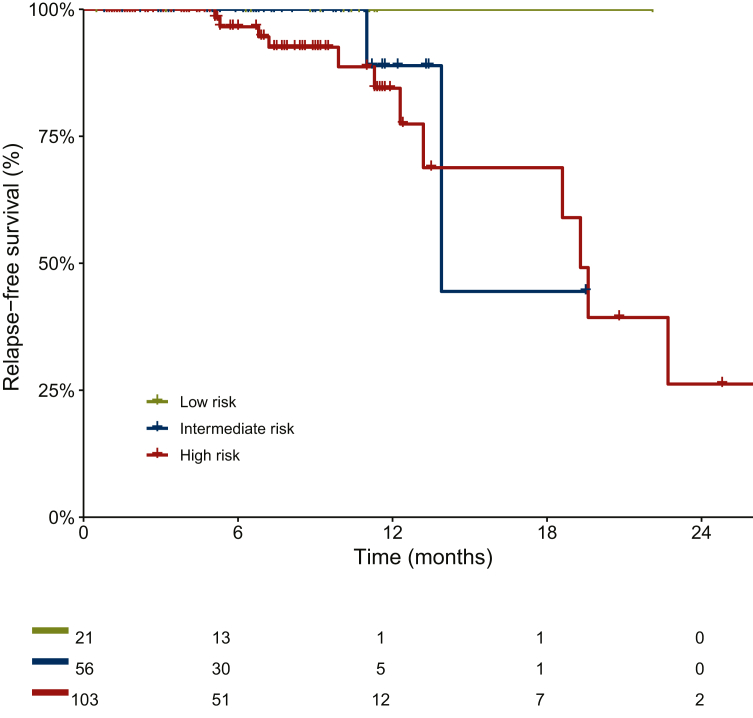
A total of 180 patients with FIGO stage I-II EOC were enrolled between January 2022 and December 2023; 126 patients (70%) had at least one ESCAT Tier I-III alteration (including 51% high risk, 35% intermediate risk, and 14% low risk); among them, approximately one-quarter (26%, 95% confidence interval 19% to 35%) had an ESCAT Tier I alteration. BRCA1 and BRCA2 alterations were observed in about one-quarter of patients, with BRCA2 often co-altered with POLE mutations (55%, P = 2.1 × 10). Notably, almost all BRCA1 variants were found in high-risk patients. BRAF V600E mutation (ESCAT IC) was found in 2.4% of patients. PIK3CA variants were the most common Tier IIIA alterations found in 59% of patients. Among those who experienced recurrence, 60% had at least one ESCAT Tier I-III alteration, with PIK3CA mutations being the most frequent.
These findings highlight the potential for actionable alterations in most early-stage EOC patients and support the exploration of chemotherapy-free regimens for low- to intermediate-risk groups, as well as targeted maintenance therapy for high-risk individuals.
根据欧洲临床肿瘤学会(ESMO)指南,早期上皮性卵巢癌(EOC)的治疗方案主要基于分级和组织学类型。对于高级别肿瘤以及国际妇产科联盟(FIGO)分期为IB-IC期的患者,通常推荐辅助化疗;然而,过度治疗仍然是一个问题。相反,目前真正具有较高复发风险的患者缺乏额外的治疗策略。
本研究对早期EOC患者进行了描述性分析,这些患者根据临床病理特征进行前瞻性测序并分为高、中、低风险组。使用OncoKB鉴定致癌改变,并根据ESMO分子靶点临床可操作性量表(ESCAT)I-III级进行分类。首先报告每个风险亚组分子检测结果的患病率,然后对复发患者队列进行分析。
2022年1月至2023年12月期间共纳入180例FIGO I-II期EOC患者;126例(70%)患者至少有一项ESCAT I-III级改变(包括51%高风险、35%中风险和14%低风险);其中,约四分之一(26%,95%置信区间19%至35%)患者有ESCAT I级改变。约四分之一的患者观察到BRCA1和BRCA2改变,BRCA2常与POLE突变共同改变(55%,P = 2.1×10)。值得注意的是,几乎所有BRCA1变异均见于高风险患者。2.4%的患者发现BRAF V600E突变(ESCAT IC)。PIK3CA变异是最常见的IIIA级改变,见于59%的患者。在复发患者中,60%至少有一项ESCAT I-III级改变,其中PIK3CA突变最为常见。
这些发现突出了大多数早期EOC患者存在可操作改变的可能性,并支持探索低至中风险组的无化疗方案以及高风险个体的靶向维持治疗。