Lukas Peter, Nilsson Lena, Wodlin Ninnie Borendal, Arendt-Nielsen Lars, Kjølhede Preben
Department of Obstetrics and Gynecology in Linköping, and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, S-581 85, Sweden.
Department of Anesthesiology and Intensive Care in Linköping, and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, S-581 85, Sweden.
BMC Womens Health. 2024 Dec 20;24(1):644. doi: 10.1186/s12905-024-03474-5.
The objectives were to determine the prevalence of de novo and persistent pelvic pain after benign hysterectomy and to assess risk factors.
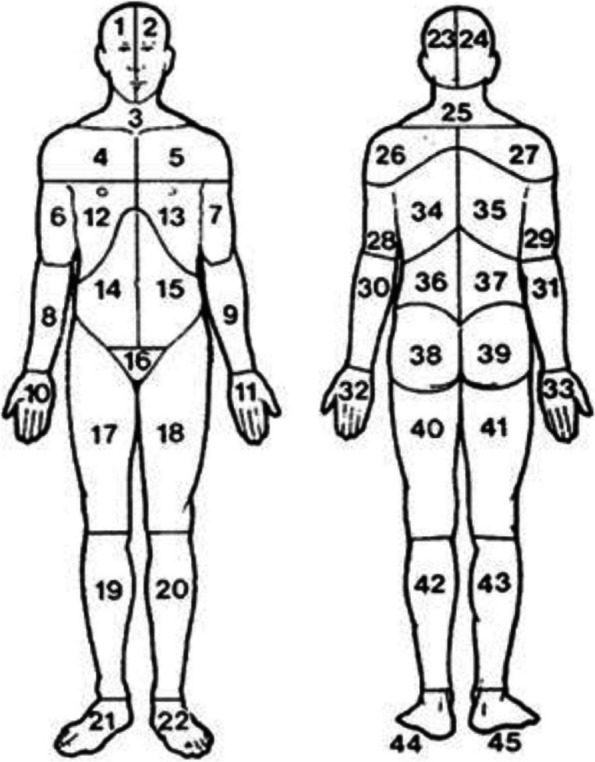
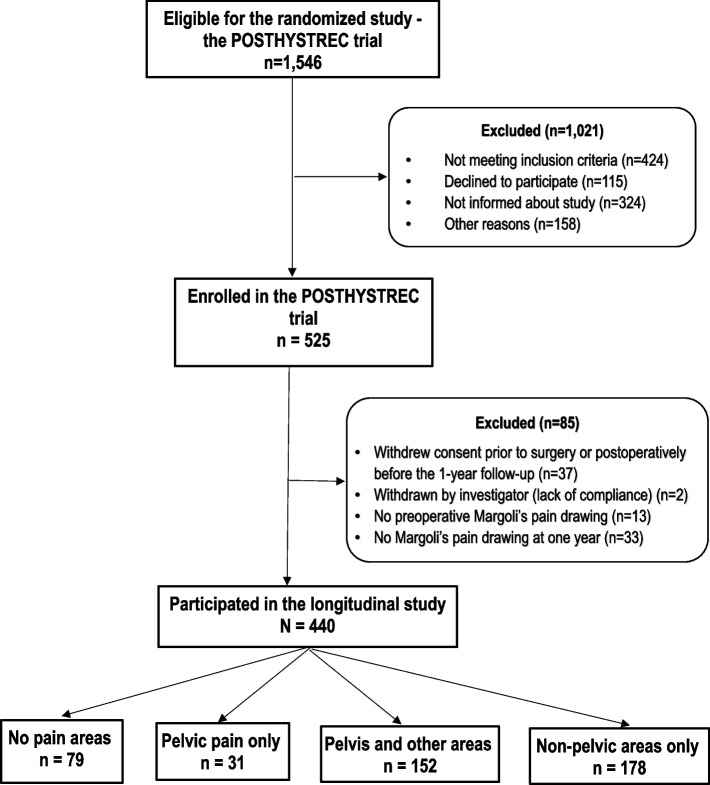
A Swedish prospective multicenter study of 440 women undergoing benign hysterectomy was conducted between October 2011 and March 2017. Measures of pain, the spatial extent of bodily pain, and pain sensitivity were assessed using a self-reporting questionnaire, Margolis's patient pain drawing, and quantitative sensory testing of pain thresholds for pressure, heat, and cold, respectively. Quality of life was evaluated by EQ-5D-3L and SF-36. Psychological distress was assessed by the Hospital Anxiety and Depression Scaleand the Stress-Coping Inventory. Logistic regression models were used to assess risk factors, and the outcome was presented as an adjusted odds ratio (aOR) and 95% confidence interval (CI).
Preoperatively, 18.0% of the women reported no bodily pain, 41.5% had pelvic pain, either as the only location (7.0%) or along with pain in other locations (34.5%), and 40.5% had non-pelvic pain only. Postoperatively, 6.2% developed de novo pelvic pain and 16.4% had persistent pelvic pain. De novo pelvic pain developed exclusively in women who preoperatively had non-pelvic pain only. Risk factors for de novo pelvic pain were a long hospital stay (aOR 1.50 (95%CI) 1.02-2.21)), high preoperative pain intensity (aOR 1.25 (95%CI 1.01-1.62)) and a high number of pain areas (aOR 1.15 (95%CI 1.05-1.27)), along with anxiety (aOR 10.61 (95%CI 1.84-61.03)) and low EQ-5D-3L health index (aOR 0.02 (95%CI 0.00-0.31)). Risk factors for persistent pelvic pain were lower age (aOR 0.89 (95%CI 0.81-0.97)), higher number of pain areas (aOR 1.08 (95%CI 1.02-1.14)), and a higher frequency of preoperative pain (aOR 12.75 (95%CI 2.24-72.66)).
Although hysterectomy appeared to be reasonably effective in curing pelvic pain, a non-negligible proportion of women developed de novo pelvic pain or had persistent pelvic pain. De novo pelvic pain seemed to affect only those who preoperatively had widespread bodily pain. Women at risk for de novo and persistent pelvic pain after hysterectomy could be identified preoperatively.
The study was retrospectively registered in ClinicalTrial.gov (NCT01526668) on 01/27//2012.
目的是确定良性子宫切除术后新发和持续性盆腔疼痛的患病率,并评估风险因素。
2011年10月至2017年3月,在瑞典对440例行良性子宫切除术的女性进行了一项前瞻性多中心研究。分别使用自我报告问卷、马戈利斯患者疼痛绘图以及压力、热和冷痛阈值的定量感觉测试,评估疼痛程度、身体疼痛的空间范围和疼痛敏感性。通过EQ-5D-3L和SF-36评估生活质量。采用医院焦虑抑郁量表和应激应对量表评估心理困扰。使用逻辑回归模型评估风险因素,结果以调整后的优势比(aOR)和95%置信区间(CI)表示。
术前,18.0%的女性报告无身体疼痛,41.5%有盆腔疼痛,其中仅盆腔疼痛(7.0%)或伴有其他部位疼痛(34.5%),40.5%仅有非盆腔疼痛。术后,6.2%出现新发盆腔疼痛,16.4%有持续性盆腔疼痛。新发盆腔疼痛仅发生在术前仅有非盆腔疼痛的女性中。新发盆腔疼痛的风险因素包括住院时间长(aOR 1.50(95%CI)1.02 - 2.21))、术前疼痛强度高(aOR 1.25(95%CI 1.01 - 1.62))和疼痛部位数量多(aOR 1.15(95%CI 1.05 - 1.27)),以及焦虑(aOR 10.61(95%CI 1.84 - 61.03))和EQ-5D-3L健康指数低(aOR 0.02(95%CI 0.00 - 0.31))。持续性盆腔疼痛的风险因素包括年龄较小(aOR 0.89(95%CI 0.81 - 0.97))、疼痛部位数量较多(aOR 1.08(95%CI 1.02 - 1.14))和术前疼痛频率较高(aOR 12.75(95%CI 2.24 - 72.66))。
尽管子宫切除术似乎在治愈盆腔疼痛方面相当有效,但仍有不可忽视比例的女性出现新发盆腔疼痛或持续性盆腔疼痛。新发盆腔疼痛似乎仅影响术前有广泛身体疼痛的女性。子宫切除术后有新发和持续性盆腔疼痛风险的女性可在术前识别。
该研究于2012年1月27日在ClinicalTrial.gov(NCT01526668)进行回顾性注册。