Luo Xiao-Xiu, Li Jia-Jia, Yang Fu-Xun, Lei Yu, Zeng Fan, Lan Yun-Ping, Pan Chun, Huang Xiao-Bo, Liu Rong-An, Luo Jing-Chao
Department of Critical Care Medicine, University of Electronic Science and Technology of China, Sichuan Academy of Medical Sciences and Sichuan Provincial People's Hospital, Chengdu, 610072, China.
Crit Care. 2024 Dec 20;28(1):426. doi: 10.1186/s13054-024-05219-0.
Perioperative airway management and oxygenation maintenance during central airway obstruction (CAO) treatment pose great challenges. While veno-venous extracorporeal membrane oxygenation (V-V ECMO) shows promise as a bridge therapy, optimal implementation and management strategies remain lacking. We present our experience with V-V ECMO in CAO management from a high-volume center.
We retrospectively analyzed 29 consecutive patients who received V-V ECMO support for CAO between 2015 and 2023. Patient demographics, clinical characteristics, ECMO cannulation and operation parameters, interventional procedures, complications, and outcomes were reviewed.
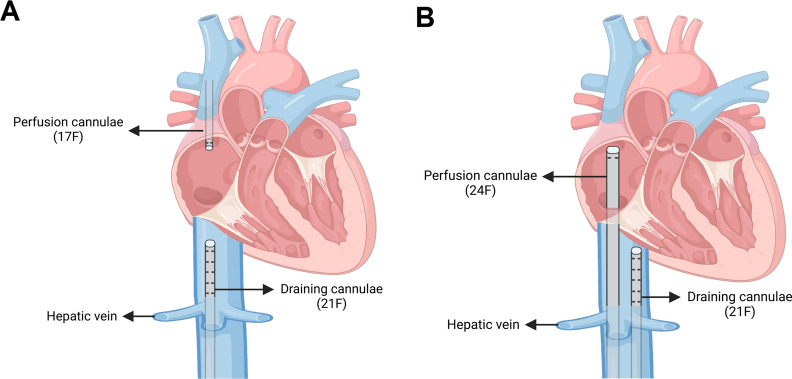
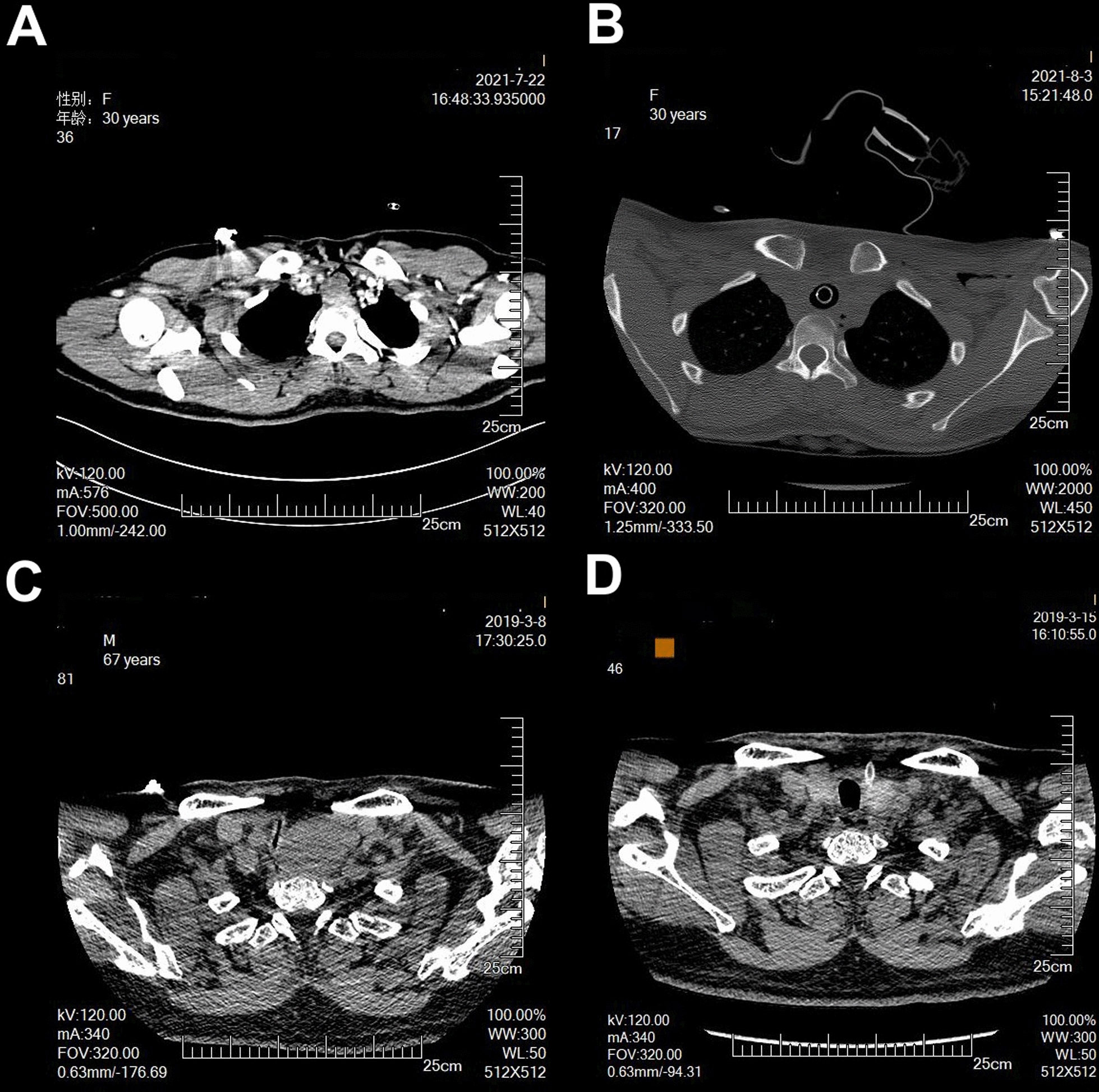
Among patients with median airway diameter of 4.5 mm (IQR 2-5 mm), etiologies included primary tumors (n = 17), metastases (n = 7), and post-intubation/tracheostomy stenosis (n = 5). Treatment comprised bronchoscopic interventions (n = 9) and surgical procedures (thoracic = 15, head/neck = 5). Using predominantly femoral-jugular cannulation (n = 27), we implemented a minimal anticoagulation protocol (catheter flush with 5U/mL heparin only). All patients survived through 6-month follow-up with minimal ECMO-related complications.
The application of V-V ECMO with minimal anticoagulation demonstrates safety and efficacy as a bridging support in the therapeutic approach to CAO.
在中央气道梗阻(CAO)治疗期间,围手术期气道管理和氧合维持面临巨大挑战。虽然静脉-静脉体外膜肺氧合(V-V ECMO)作为一种桥接治疗显示出前景,但仍缺乏最佳的实施和管理策略。我们介绍了我们在一家高容量中心使用V-V ECMO管理CAO的经验。
我们回顾性分析了2015年至2023年间连续接受V-V ECMO支持治疗CAO的29例患者。回顾了患者的人口统计学、临床特征、ECMO插管和操作参数、介入程序、并发症及结局。
气道直径中位数为4.5mm(四分位间距2-5mm)的患者中,病因包括原发性肿瘤(n = 17)、转移瘤(n = 7)和插管/气管切开术后狭窄(n = 5)。治疗包括支气管镜干预(n = 9)和外科手术(胸部 = 15,头/颈部 = 5)。主要采用股静脉-颈内静脉插管(n = 27),我们实施了最小化抗凝方案(仅用5U/mL肝素冲洗导管)。所有患者均存活至6个月随访期,ECMO相关并发症极少。
应用最小化抗凝的V-V ECMO作为CAO治疗方法中的桥接支持显示出安全性和有效性。