Zhao Yang-Chao, Zhao Xi, Fu Guo-Wei, Huang Ming-Jun, Li Xing-Xing, Sun Qian-Qian, Kan Ya-Bai, Li Jun, Wang Shi-Lei, Ma Wen-Tao, Xu Qin-Fu, Liu Qi-Long, Li Hong-Bin
Department of Extracorporeal Life Support Center, Department of Cardiac Surgery, The First Affiliated Hospital of Zhengzhou University, JianShe Road 1, Zhengzhou, 450052, Henan, China.
Department of Cardiology, Henan Key Laboratory of Hereditary Cardiovascular Diseases, The First Affiliated Hospital of Zhengzhou University, Cardiovascular Center, Zhengzhou, 450052, Henan, China.
Thromb J. 2022 Jun 27;20(1):36. doi: 10.1186/s12959-022-00396-w.
The anti-coagulation protocol of patients with hemorrhage risk primary disease who need extracorporeal membrane oxygenation (ECMO) supported is controversial. This study evaluated the feasibility of a new anti-coagulation strategy, that is heparin-free after 3000 IU heparin loaded in veno-venous ECMO (VV ECMO) supported acute respiratory failure patients with hemorrhage risk.
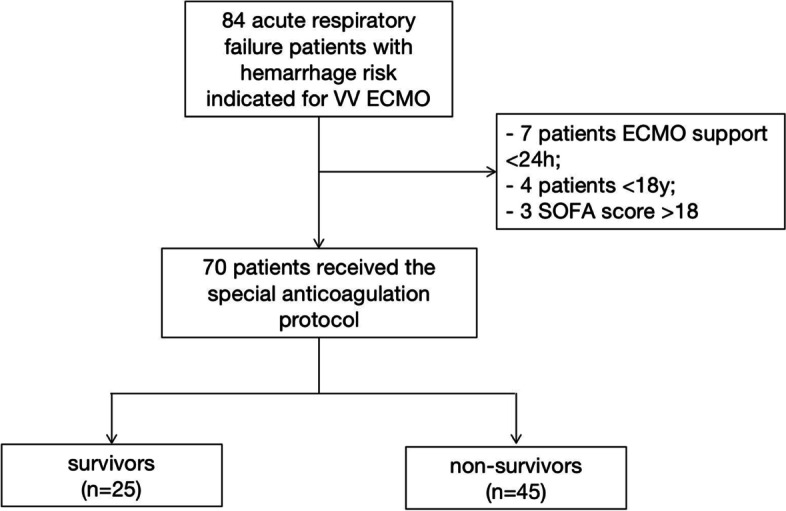
A retrospective study was performed in a series of hemorrhage risk patients supported with VV ECMO at the First Affiliated Hospital of Zhengzhou University, between June 2012 to Sept 2020. A total of 70 patients received a low heparin bolus of 3000 units for cannulation but without subsequent, ongoing heparin administration. Patients were divided into survival (n = 25) and non-survival group (n = 45). Data of coagulation, hemolysis and membrane lung function were calculated and analyzed. The complications of patients were recorded. Finally, the binary Logistic regression was conducted.
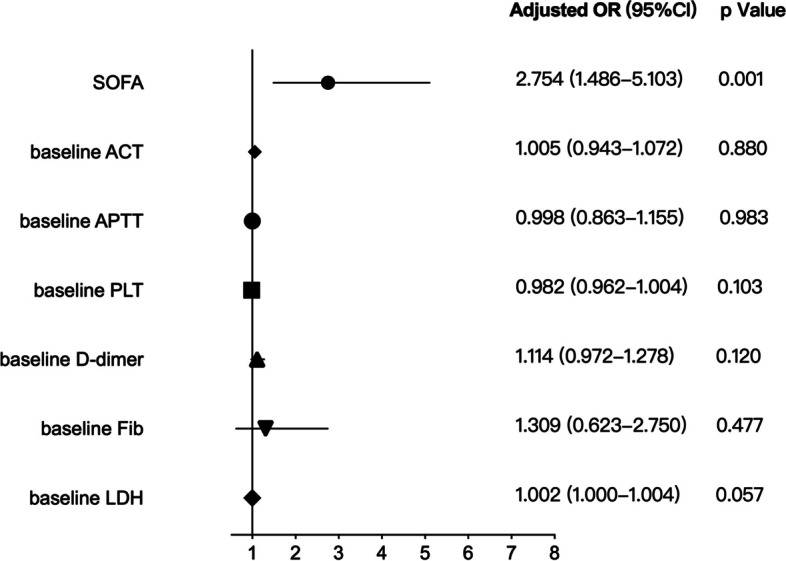
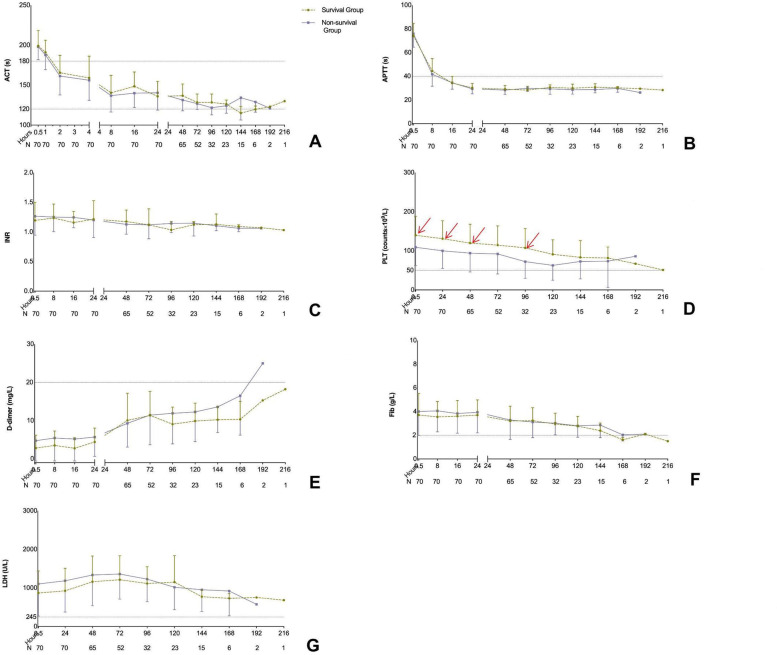
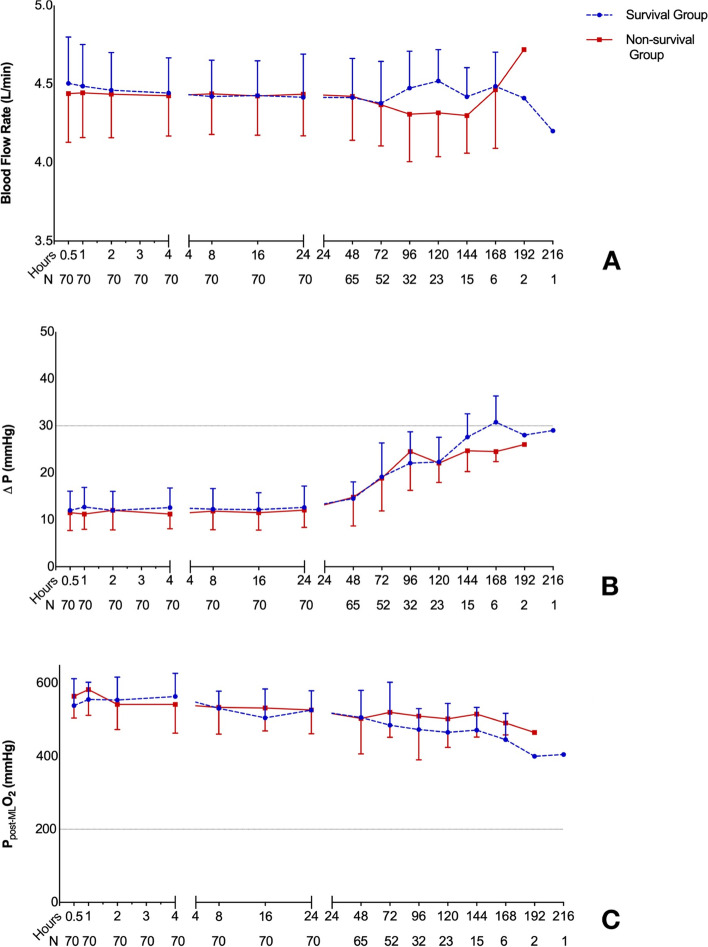
The longest heparin-free time was 216 h, and the mean heparin-free time was 102 h. Compared with survivors, the non-survivors were showed higher baseline SOFA score and lower platelet counts in 0.5 h, 24 h, 48 h and 96 h after ECMO applied. However, there was no significant differences between survivors and non-survivors in ACT, APTT, INR, D-dimer, fibrinogen, LDH, blood flow rate, Δp and PO (all p < 0.05) of all different time point. Moreover, only the baseline SOFA score was significantly associated with mortality (p < 0.001, OR(95%CI): 2.754 (1.486-5.103)) while the baseline levels of ACT, APTT, INR, platelet, D-dimer, fibrinogen and LDH have no association with mortality. The percentage of thrombosis complications was 54.3% (38/70) including 3 oxygenator changed but there was no significant difference of complications in survival and non-survival groups (p > 0.05).
The anticoagulation protocol that no heparin after a 3000 units heparin bolus in VV ECMO supported acute respiratory failure patients with hemorrhage risk is feasible.
对于有出血风险的原发性疾病且需要体外膜肺氧合(ECMO)支持的患者,其抗凝方案存在争议。本研究评估了一种新的抗凝策略的可行性,即在静脉 - 静脉ECMO(VV ECMO)支持的有出血风险的急性呼吸衰竭患者中,给予3000 IU肝素负荷量后不再使用肝素。
对2012年6月至2020年9月在郑州大学第一附属医院接受VV ECMO支持的一系列有出血风险的患者进行回顾性研究。共有70例患者在置管时接受了3000单位的低剂量肝素推注,但随后未持续给予肝素。患者分为生存组(n = 25)和非生存组(n = 45)。计算并分析凝血、溶血和膜肺功能数据。记录患者的并发症。最后进行二元Logistic回归分析。
最长无肝素时间为216小时,平均无肝素时间为102小时。与幸存者相比,非幸存者在应用ECMO后0.5小时、24小时、48小时和96小时的基线序贯器官衰竭评估(SOFA)评分更高,血小板计数更低。然而,在所有不同时间点的活化凝血时间(ACT)、活化部分凝血活酶时间(APTT)、国际标准化比值(INR)、D - 二聚体、纤维蛋白原、乳酸脱氢酶(LDH)、血流速度、跨膜压差(Δp)和氧分压(PO)方面,幸存者和非幸存者之间无显著差异(所有p < 0.05)。此外,只有基线SOFA评分与死亡率显著相关(p < 0.001,比值比(95%可信区间):2.754(1.486 - 5.103)),而ACT、APTT、INR、血小板、D - 二聚体、纤维蛋白原和LDH的基线水平与死亡率无关。血栓形成并发症的发生率为54.3%(38/70),包括3次更换氧合器,但生存组和非生存组的并发症无显著差异(p > 0.05)。
在VV ECMO支持的有出血风险的急性呼吸衰竭患者中,给予3000单位肝素推注后不再使用肝素的抗凝方案是可行的。