Carlson Aaron M, Sollero Carlos E V, Wolf Andrew B, Sillau Stefan, Schmitt Barrie L, Money Kelli M, Nair Kavita V, Piquet Amanda L, Bennett Jeffrey L
Department of Neurology, University of Colorado School of Medicine, Aurora, Colorado, USA.
Department of Neurology, University of Rochester, Rochester, New York, USA.
Ann Clin Transl Neurol. 2025 Jan;12(1):169-179. doi: 10.1002/acn3.52268. Epub 2024 Dec 21.
To define the epidemiology and clinical presentation of seropositive neuromyelitis optica spectrum disorder (NMOSD) in a large US health system.
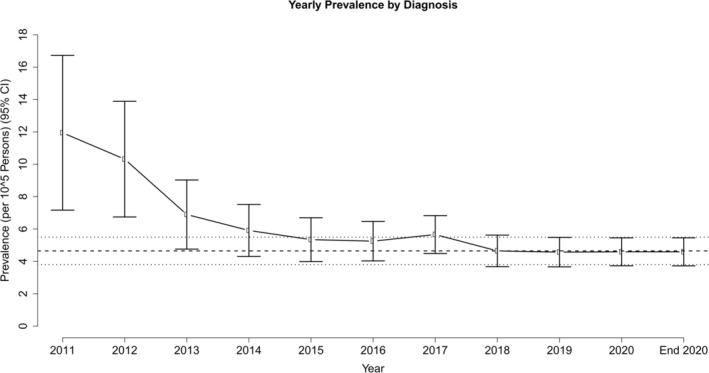
We completed a retrospective observational study of adult patients in the University of Colorado Health System from 1 January 2011 to 31 December 2020, using Health Data Compass (HDC), a data warehouse that combines electronic health information with claims and public health data in Colorado. We screened HDC for patients with either (1) an abnormal aquaporin-4 IgG test or (2) any G36 ICD-10 code. We extracted key clinical elements by chart review and confirmed diagnosis by the 2015 International Panel for NMO Diagnosis criteria. Annual incidence and prevalence rates were calculated.
Our population consisted of 2,475,591 individuals contributing 11,103,522.72 person-years of observation. In total, 115 seropositive NMOSD patients were identified. The average yearly incidence was 0.22 per 100,000 person-years. Age and sex-adjusted prevalence (per 100,000) was 4.33, and highest among those identifying as Asian or Pacific Islander (17.72), and Black (14.74), as separately by Hispanic ethnicity (8.02). Prevalence was higher in women (6.20:1 female:male ratio). Transverse myelitis (45%) and optic neuritis (43%) were the most common presenting clinical syndromes. In total, 6% of initial presentations were characterized by short-segment transverse myelitis without other features.
Seropositive NMOSD incidence is higher in our cohort than many contemporary studies. Women and those identifying as Asian or Pacific Islander, Black, and Hispanic shoulder the highest burden of disease. Clinical onset with short-segment myelitis underscores the need for serum aquaporin-4 IgG testing in acute myelitis presentations.
确定美国一个大型医疗系统中血清学阳性的视神经脊髓炎谱系障碍(NMOSD)的流行病学特征和临床表现。
我们对科罗拉多大学医疗系统2011年1月1日至2020年12月31日期间的成年患者进行了一项回顾性观察研究,使用健康数据指南针(HDC),这是一个将电子健康信息与科罗拉多州的理赔和公共卫生数据相结合的数据仓库。我们在HDC中筛选符合以下任一条件的患者:(1)水通道蛋白4 IgG检测异常;(2)任何G36 ICD-10编码。我们通过病历审查提取关键临床要素,并根据2015年国际视神经脊髓炎诊断小组标准确诊。计算年发病率和患病率。
我们的研究人群包括2475591人,观察时长为11103522.72人年。总共识别出115例血清学阳性的NMOSD患者。年平均发病率为每10万人年0.22例。年龄和性别调整后的患病率(每10万人)为4.33,按西班牙裔种族分别划分,在亚洲或太平洋岛民(17.72)和黑人(14.74)中患病率最高,西班牙裔为(8.02)。女性患病率更高(女性与男性比例为6.20:1)。横贯性脊髓炎(45%)和视神经炎(43%)是最常见的首发临床综合征。总共有6%的首发表现为无其他特征的短节段横贯性脊髓炎。
在我们的队列中,血清学阳性的NMOSD发病率高于许多当代研究。女性以及亚洲或太平洋岛民、黑人、西班牙裔人群疾病负担最重。急性脊髓炎表现为短节段脊髓炎的临床发病情况凸显了在急性脊髓炎表现中进行血清水通道蛋白4 IgG检测的必要性。