Liu Jian-Jun, Zheng Huili, Liu Sylvia, Kwan Tsz Kiu, Gurung Resham L, Chan Clara, Lee Janus, Ang Keven, de Keizer Joe, Hadjadj Samy, Saulnier Pierre-Jean, Chong Mary F F, Lim Su Chi
Clinical Research Unit, Khoo Teck Puat Hospital, Singapore, 768828, Republic of Singapore.
L'institut du Thorax, INSERM, CNRS, UNIV Nantes, CHU Nantes, Nantes, France.
Cardiovasc Diabetol. 2024 Dec 21;23(1):451. doi: 10.1186/s12933-024-02546-y.
Data on the relationship between potassium intake and major cardiovascular events (MACE) in patients with diabetes are scarce. We aim to study the association between estimated potassium intake and risk of MACE in individuals with type 2 diabetes.
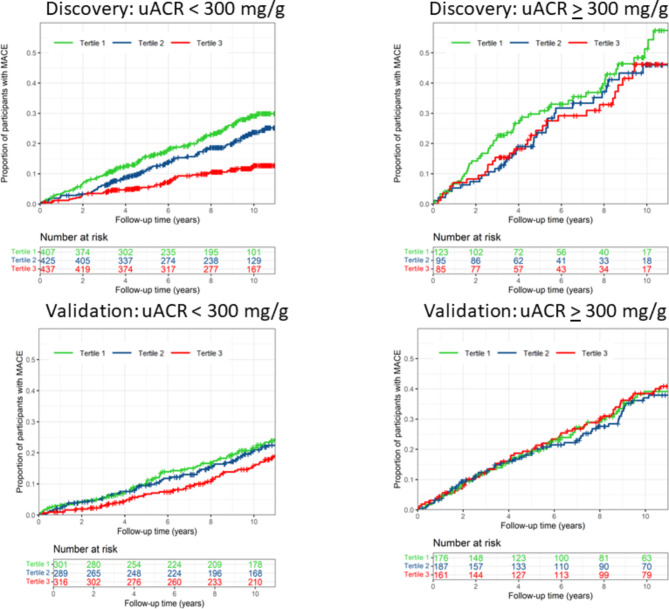
The discovery cohort consisted of 1572 participants with type 2 diabetes from a secondary hospital. The validation cohort consisted of 1430 participants with diabetes from a multicenter study (Chronic Renal Insufficiency Cohort, CRIC). Potassium intake was estimated from potassium in spot urine using Kawasaki formula and in 24-h urine collection in two cohorts, respectively. The primary outcome was MACE defined as a composite of myocardial infarction, stroke and cardiovascular death.
During a median of 8.2 years of follow-up, 341 MACE events were identified in discovery cohort. Compared to the lowest tertile, participants with potassium intake in the top tertile had 34% lower risk for MACE after adjustment for cardio-renal risk factors (adjusted hazard ratio, aHR [95% CI], 0.66 [0.49-0.89]). This inverse association was more pronounced in participants with normal or moderately elevated albuminuria as compared to those with severely elevated albuminuria (urine albumin-to-creatinine ratio > 300 mg/g, p for interaction < 0.05). In consistence, a higher potassium intake was independently associated with a lower risk of MACE in CRIC participants with diabetes and moderately elevated albuminuria (aHR 0.61 [0.42-0.90], top vs. lowest tertile).
A high level potassium intake estimated from urine potassium excretion was independently associated with a low risk of MACE in patients with type 2 diabetes. Increasing potassium intake may be a potential effective strategy for cardiovascular risk reduction beyond controlling traditional risk factors.
关于糖尿病患者钾摄入量与主要心血管事件(MACE)之间关系的数据稀少。我们旨在研究2型糖尿病患者估计的钾摄入量与MACE风险之间的关联。
发现队列由一家二级医院的1572名2型糖尿病参与者组成。验证队列由一项多中心研究(慢性肾功能不全队列,CRIC)中的1430名糖尿病参与者组成。分别使用川崎公式根据即时尿中的钾以及两个队列中24小时尿钾收集量来估计钾摄入量。主要结局是MACE,定义为心肌梗死、中风和心血管死亡的复合事件。
在中位8.2年的随访期间,发现队列中识别出341例MACE事件。与最低三分位数相比,钾摄入量处于最高三分位数的参与者在调整心血管肾脏危险因素后发生MACE的风险降低34%(调整后风险比,aHR [95% CI],0.66 [0.49 - 0.89])。与白蛋白尿严重升高(尿白蛋白与肌酐比值>300 mg/g)的参与者相比,这种负相关在白蛋白尿正常或中度升高的参与者中更为明显(交互作用p<0.05)。同样,在CRIC队列中糖尿病且白蛋白尿中度升高的参与者中,较高的钾摄入量与较低的MACE风险独立相关(aHR 0.61 [0.42 - 0.90],最高三分位数与最低三分位数相比)。
根据尿钾排泄量估计的高水平钾摄入量与2型糖尿病患者发生MACE的低风险独立相关。增加钾摄入量可能是一种潜在的有效策略,可在控制传统危险因素之外降低心血管风险。