Peng Weicheng, Xiang Xinli, Li Zhehong, Zhao Rui, Liang Xin, Guan Feng, Hu Zhiqiang
Department of Neurosurgery, Neuromedicine Center, Beijing Shijitan Hospital, Capital Medical University, No. 10, Tieyi Road, Yangfangdian, Haidian District, Beijing, 100038, People's Republic of China.
Department of Pharmacy, Beijing Shijitan Hospital, Capital Medical University, No. 10, Tieyi Road, Yangfangdian, Haidian District, Beijing, 100038, People's Republic of China.
Eur J Med Res. 2024 Dec 23;29(1):613. doi: 10.1186/s40001-024-02205-8.
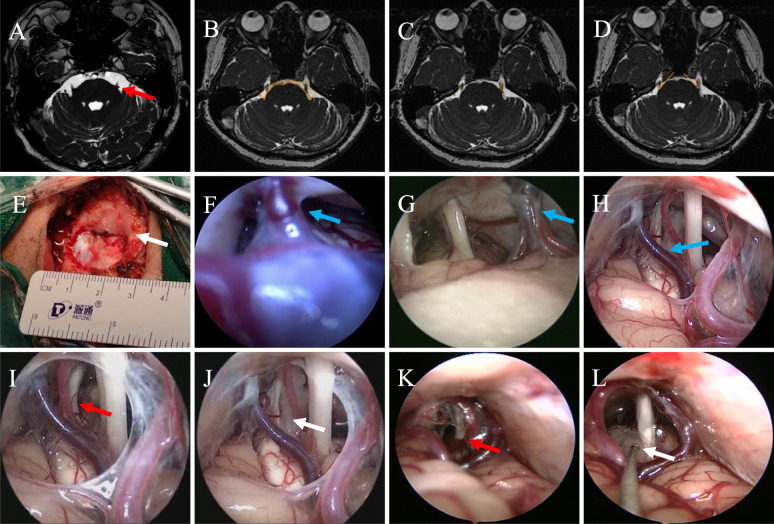
Full-endoscopic microvascular decompression (fE-MVD) is an emerging treatment option for trigeminal neuralgia (TN). However, the risk factors associated with postoperative recurrence of TN after fE-MVD procedure remain controversial. The aim of the present study was to summarize the surgical technique of fE-MVD for the treatment of TN and to develop a predictive model for recurrence at 1 year postoperatively based on independent risk factors.
A total of 124 consecutive patients with TN who underwent fE-MVD procedure were enrolled in this study between December 2008 and July 2022. Imaging data such as the area of cerebellopontine angle (CPA), the length of trigeminal cisternal segment, and the angle of trigeminal nerve (TGN) were measured from preoperative magnetic resonance imaging (MRI). Patients were randomly divided into a training set and a validation set according to the 7:3 ratio, respectively. Variables that were significant in the univariate logistic analyses were, subsequently, included in the multivariate logistic regression analyses in training set. Then, we developed a predictive nomogram for the 1-year recurrence of TN for patients who treated with fE-MVD.
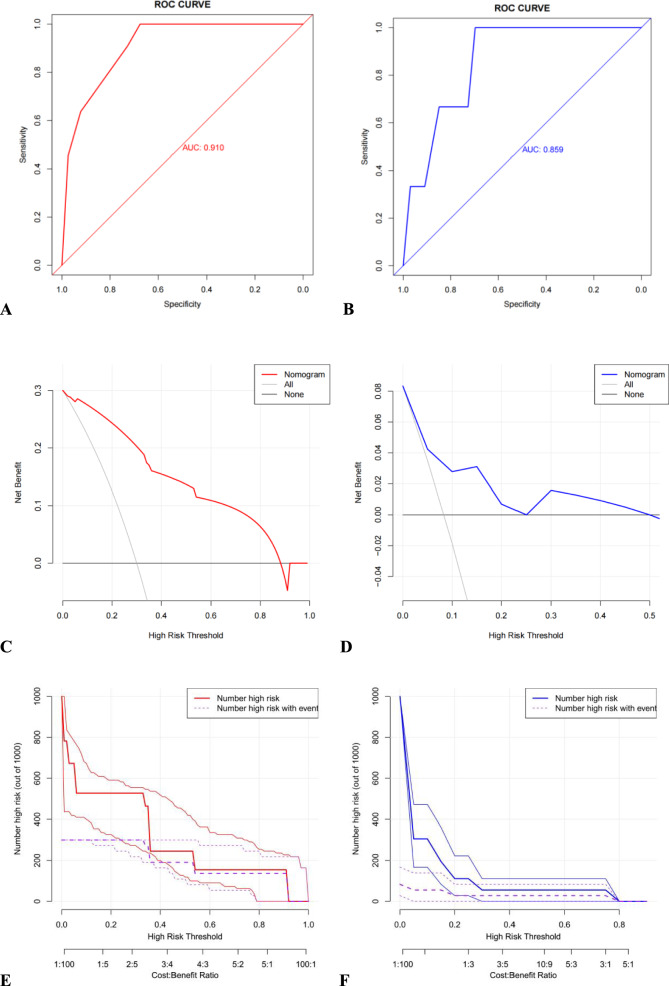
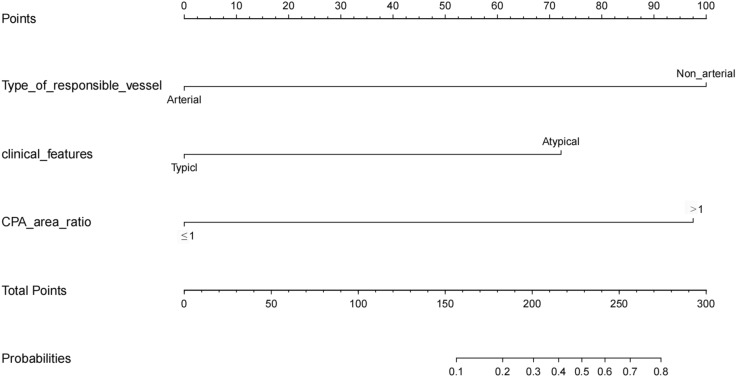
All 124 patients experienced clinically significant pain relief (Barrow Neurology Institute (BNI) I-II) after fE-MVD. 124 patients had a follow-up time of more than 1 year, with 14 cases of recurrence. In the univariate analysis, the patients' responsible vessels of non-arterial, clinical features of atypical, and CPA area ratio (healthy/affected side) >1 were found to be significantly associated with recurrence of TN after fE-MVD. Multivariate logistic regression analyses result showed that the patients' responsible vessels of non-arterial (odds ratio (OR) = 21.067, 95% confidence interval (CI): 1.942-228.575), clinical features of atypical (OR = 9.027, 95% CI: 1.135-71.777), and CPA area ratio >1 (OR = 19.522, 95% CI: 2.906-131.160) were independent predictors of TN recurrence. Based on the independent predictive factors, we developed a predictive nomogram that predicts the 1-year recurrence of TN after fE-MVD. In the receiver operating characteristic (ROC) curve analysis, the area under the curve (AUC) of the nomograms for 1-year recurrence associated with optimal candidates prediction was 0.910 in the training set and 0.859 in the validation set.
FE-MVD for the treatment of TN is a safe, reliable and effective procedure. Patients' responsible vessels of non-arterial, clinical features of atypical, and CPA area ratio (healthy/affected side) >1 are key risk factors associated with 1 year postoperative recurrence of TN after fE-MVD. Finally, we have developed a nomogram to predict the 1-year recurrence of TN for patients who treated with fE-MVD, which can be used to provide advice for patients after fE-MVD.
全内镜下微血管减压术(fE-MVD)是治疗三叉神经痛(TN)的一种新兴治疗选择。然而,fE-MVD术后TN复发的相关危险因素仍存在争议。本研究的目的是总结fE-MVD治疗TN的手术技术,并基于独立危险因素建立术后1年复发的预测模型。
2008年12月至2022年7月期间,共有124例连续接受fE-MVD手术的TN患者纳入本研究。术前磁共振成像(MRI)测量桥小脑角(CPA)面积、三叉神经脑池段长度和三叉神经(TGN)角度等影像数据。患者按7:3的比例随机分为训练集和验证集。单因素逻辑分析中有统计学意义的变量随后纳入训练集的多因素逻辑回归分析。然后,我们为接受fE-MVD治疗的患者建立了TN 1年复发的预测列线图。
所有124例患者在fE-MVD术后均有临床显著的疼痛缓解(巴罗神经学研究所(BNI)I-II级)。124例患者随访时间超过1年,其中14例复发。单因素分析发现,非动脉性责任血管、非典型临床特征以及CPA面积比(健侧/患侧)>1与fE-MVD术后TN复发显著相关。多因素逻辑回归分析结果显示,非动脉性责任血管(比值比(OR)=21.067,95%置信区间(CI):1.942-228.575)、非典型临床特征(OR = 9.027,95% CI:1.135-71.777)和CPA面积比>1(OR = 19.522,95% CI:2.906-131.160)是TN复发的独立预测因素。基于这些独立预测因素,我们建立了一个预测列线图,用于预测fE-MVD术后TN的1年复发情况。在受试者工作特征(ROC)曲线分析中,训练集中与最佳候选预测相关的1年复发列线图曲线下面积(AUC)为0.910,验证集中为0.859。
fE-MVD治疗TN是一种安全、可靠且有效的手术。非动脉性责任血管、非典型临床特征以及CPA面积比(健侧/患侧)>1是fE-MVD术后TN 1年复发的关键危险因素。最后,我们建立了一个列线图来预测接受fE-MVD治疗患者的TN 1年复发情况,可为fE-MVD术后患者提供建议。