Ramirez Oscar, Piedrahita Vivian, Bolivar Santiago, Grillo Karina, Linares Adriana, Pardo Carlos, Piña Martha, Suarez Amaranto, Portilla Carlos A, Ardila Jesus, Lotero Viviana, Urcuqui Luz A, Trujillo Angela, Montenegro Patricia, Bravo Luis E, Aristizabal Paula
Fundación POHEMA, Unidad de Investigación, Cali, Colombia.
Clínica Imbanaco-Grupo Quirón Salud, Unidad de Oncología y Hematología Pediátrica, Cali, Colombia.
Cancer Med. 2024 Dec;13(24):e70483. doi: 10.1002/cam4.70483.
Measures to control COVID-19 transmission disrupted childhood cancer care. Data on the effects of the COVID-19 pandemic on childhood cancer mortality are lacking. This study describes the impact of the pandemic on childhood cancer early-mortality (≤ 24 months).
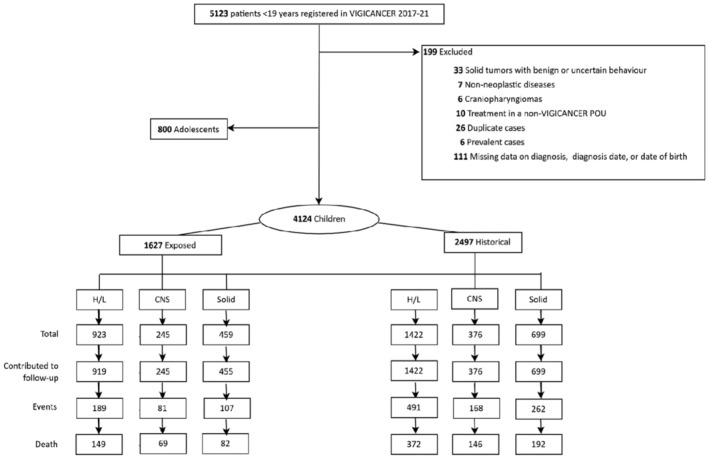
A multicenter prospective cohort was conducted in 10 Colombian cities. Children with newly diagnosed cancer registered in the Childhood Cancer Clinical Outcomes Surveillance System (VIGICANCER) were included. Our primary outcome was cumulative mortality at 3, 6, 12, and 24 months. The exposed cohort (EC = March 25, 2020-December 31, 2021) was compared with a historic cohort (HC = January 1, 2017-March 24, 2020). Covariates included sociodemographics, place of residence, health insurance type, and tumor classification.
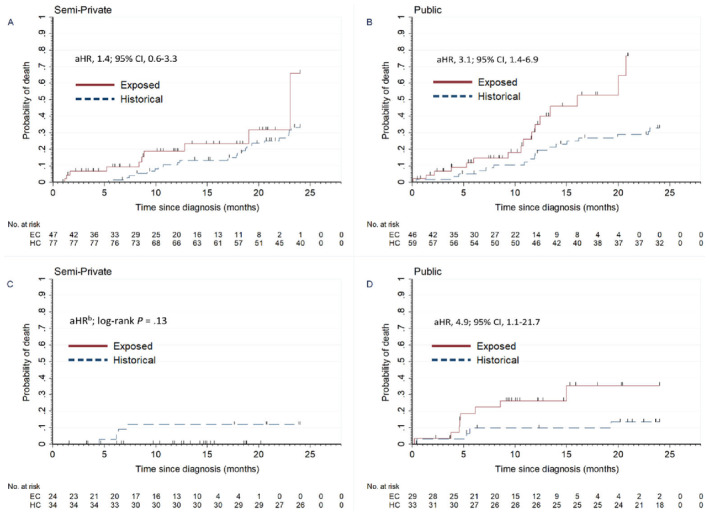
The cohort included 4124 children, comprised of 1627 children in the EC and 2497 children in the HC. Hematolymphoid, central nervous system, and extracranial solid tumors represented 57%, 15%, and 28% of patients, respectively. Participants' median age was 6.7 years (IQR, 3.2-11.3), 54% were male, 7% were Afro-descendant, and 47% had public insurance. In the EC, the 6-month and 24-month mortality adjusted hazard ratio (aHR) in children with solid tumors was 1.7 (95% CI, 1.1-2.7) and 1.3 (95% CI, 1.0-1.7), respectively, and in children with bone tumors 4.0 (95% CI, 1.2-13.0) and 2.1 (95% CI, 1.2-3.6), respectively. These associations persisted after accounting for metastatic disease. Six-month mortality aHRs for retinoblastoma, bone tumors, and soft tissue sarcomas due to progressive disease were 4.3 (95% CI, 1.3-14.5), 4.0 (95% CI, 1.4-11.3), and 5.4 (95% CI, 2.2-13.5), respectively. In the EC, the adjusted odds ratio (aOR) for metastatic solid tumors vs. nonmetastatic was 1.4 (95% CI, 1.0-1.8) and in children with retinoblastoma and public insurance the 24-month mortality aHR was 4.9 (95% CI, 1.1-21.7).
We observed increased early-mortality for solid tumors, particularly bone tumors and retinoblastoma, likely attributed to more advanced-stage presentation and loss of treatment effectiveness due to healthcare disruptions. Early-mortality was higher in patients with public insurance, a vulnerable population that warrants attention.
控制新冠病毒传播的措施扰乱了儿童癌症护理。缺乏关于新冠疫情对儿童癌症死亡率影响的数据。本研究描述了疫情对儿童癌症早期死亡率(≤24个月)的影响。
在哥伦比亚的10个城市进行了一项多中心前瞻性队列研究。纳入在儿童癌症临床结局监测系统(VIGICANCER)中登记的新诊断癌症儿童。我们的主要结局是3、6、12和24个月时的累积死亡率。将暴露队列(EC = 2020年3月25日至2021年12月31日)与历史队列(HC = 2017年1月1日至2020年3月24日)进行比较。协变量包括社会人口统计学、居住地点、健康保险类型和肿瘤分类。
该队列包括4124名儿童,其中EC组1627名儿童,HC组2497名儿童。血液淋巴系统、中枢神经系统和颅外实体瘤分别占患者的57%、15%和28%。参与者的中位年龄为6.7岁(四分位间距,3.2 - 11.3),54%为男性,7%为非裔,47%拥有公共保险。在EC组中,实体瘤儿童6个月和24个月死亡率的调整后风险比(aHR)分别为1.7(95%置信区间,1.1 - 2.7)和1.3(95%置信区间,1.0 - 1.7),骨肿瘤儿童分别为4.0(95%置信区间,1.2 - 13.0)和2.1(95%置信区间,1.2 - 3.6)。在考虑转移性疾病后,这些关联仍然存在。视网膜母细胞瘤、骨肿瘤和软组织肉瘤因疾病进展导致的6个月死亡率aHR分别为4.3(95%置信区间,1.3 - 14.5)、4.0(95%置信区间,1.4 - 11.3)和5.4(95%置信区间,2.2 - 13.5)。在EC组中,转移性实体瘤与非转移性实体瘤的调整后比值比(aOR)为1.4(95%置信区间,1.0 - 1.8),在拥有公共保险的视网膜母细胞瘤儿童中,24个月死亡率aHR为4.9(95%置信区间,1.1 - 21.7)。
我们观察到实体瘤,特别是骨肿瘤和视网膜母细胞瘤的早期死亡率增加,这可能归因于疾病分期更晚以及医疗保健中断导致治疗效果丧失。公共保险患者的早期死亡率更高,这一弱势群体值得关注。