Calderon Adam, Irwin Matthew, Simon Naomi M, Shear M Katherine, Mauro Christine, Zisook Sidney, Reynolds Charles F, Malgaroli Matteo
Department of Psychiatry, New York University Grossman School of Medicine, New York, New York.
Department of Psychology, The Pennsylvania State University, University Park, Pennsylvania.
medRxiv. 2024 Dec 12:2024.12.11.24318861. doi: 10.1101/2024.12.11.24318861.
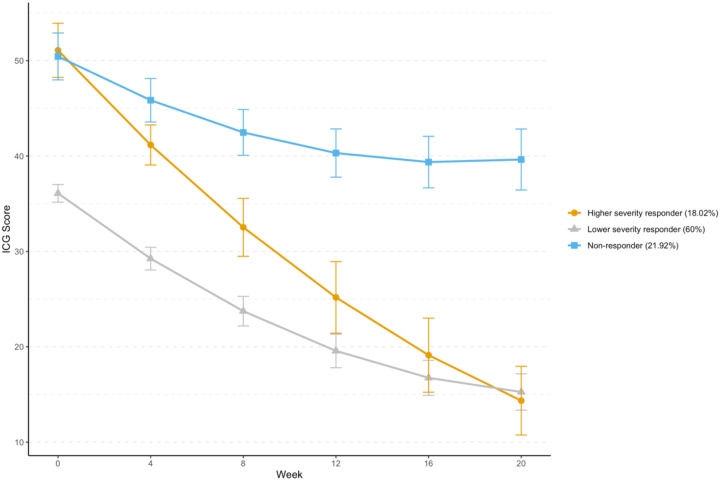
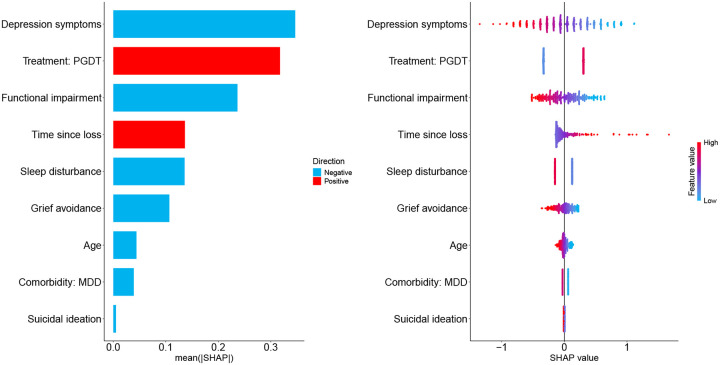
Although evidence-based treatments for Prolonged Grief Disorder (PGD) exist, pretreatment characteristics associated with differential improvement trajectories have not been identified. To identify clinical factors relevant to optimizing PGD treatment outcomes, we used unsupervised and supervised machine learning to study treatment effects from a double-blinded, placebo-controlled, randomized clinical trial. Participants were randomized into four treatment groups for 20 weeks: citalopram with grief-informed clinical management, citalopram with prolonged grief disorder therapy (PGDT), pill placebo with PGDT, or pill placebo with clinical management. The trial included 333 PGD patients aged 18-95 years ( = 53.9; ± 14.4), predominantly female (77.4%) and white (84.4%). Symptom trajectories were assessed using latent growth mixture modeling based on Inventory for Complicated Grief scores collected at six time points every 4 weeks. The relationship between patient-level characteristics and assigned trajectories was examined using logistic regression with elastic net regularization based on the administration of citalopram, PGDT, and risk factors for developing PGD. Three distinct response trajectories were identified: lesser severity responders (60%, n = 200), greater severity responders (18.02%, n = 60), and non-responders (21.92%, n = 73). Differences between greater severity responders and non-responders emerged as statistically significant by Week 8. The elastic net model demonstrated acceptable discrimination between responders and non-responders (AUC = .702; accuracy = .684). Higher baseline depression severity, grief-related functional impairment, and absence of PGDT were associated with reduced treatment response likelihood. These findings underscore the importance of early identification of clinical factors to optimize individualized PGD treatment strategies.
clinicaltrials.gov Identifier: NCT01179568.
尽管存在基于证据的持续性悲伤障碍(PGD)治疗方法,但尚未确定与不同改善轨迹相关的治疗前特征。为了确定与优化PGD治疗结果相关的临床因素,我们使用无监督和有监督的机器学习方法,对一项双盲、安慰剂对照、随机临床试验的治疗效果进行了研究。参与者被随机分为四个治疗组,为期20周:西酞普兰联合悲伤知情临床管理、西酞普兰联合持续性悲伤障碍治疗(PGDT)、安慰剂联合PGDT、或安慰剂联合临床管理。该试验纳入了333名年龄在18 - 95岁之间的PGD患者(平均年龄 = 53.9岁;标准差 ± 14.4),主要为女性(77.4%)和白人(84.4%)。使用基于每4周收集的复杂悲伤量表得分的潜在增长混合模型来评估症状轨迹。基于西酞普兰、PGDT的使用情况以及发生PGD的风险因素,采用带有弹性网正则化的逻辑回归分析,研究患者水平特征与分配轨迹之间的关系。确定了三种不同的反应轨迹:症状较轻的反应者(60%,n = 200)、症状较重的反应者(18.02%,n = 60)和无反应者(21.92%,n = 73)。到第8周时,症状较重的反应者和无反应者之间的差异在统计学上具有显著性。弹性网模型在反应者和无反应者之间表现出可接受的区分能力(曲线下面积 = 0.702;准确率 = 0.684)。较高的基线抑郁严重程度、与悲伤相关的功能损害以及未接受PGDT与治疗反应可能性降低相关。这些发现强调了早期识别临床因素以优化个体化PGD治疗策略的重要性。
clinicaltrials.gov标识符:NCT01179568。