Aljiffry Alaa, Harriott Ashley, Patel Shayli, Scheel Amy, Amedi Alan, Evans Sean, Xiang Yijin, Harding Amanda, Shashidharan Subhadra, Beshish Asaad G
Department of Pediatrics, Division of Cardiology, Emory University School of Medicine, Children's Healthcare of Atlanta, Atlanta, GA, USA.
Emory University School of Medicine, Atlanta, GA, USA.
Int J Cardiol Congenit Heart Dis. 2024 Jul 26;17:100533. doi: 10.1016/j.ijcchd.2024.100533. eCollection 2024 Sep.
The Norwood operation (NO) for infants with univentricular physiology has high interstage mortality. This study evaluated outcomes and risk factors for mortality following NO.
Retrospective single-center study of patients undergoing NO from 2010 to 2020. Analysis used appropriate statistics.
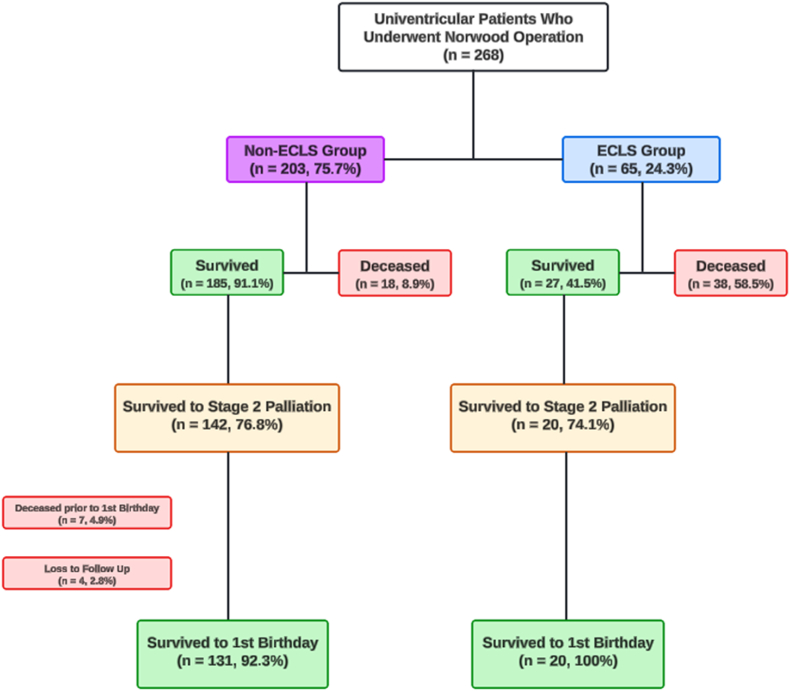
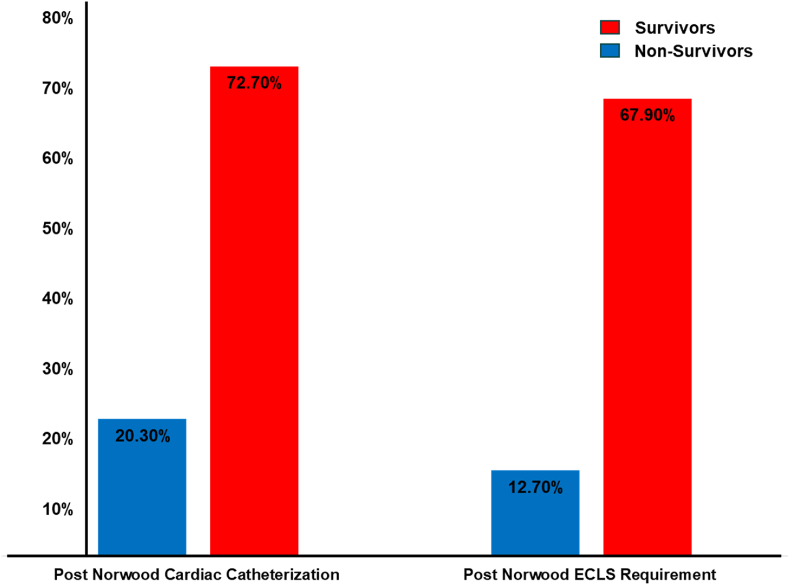
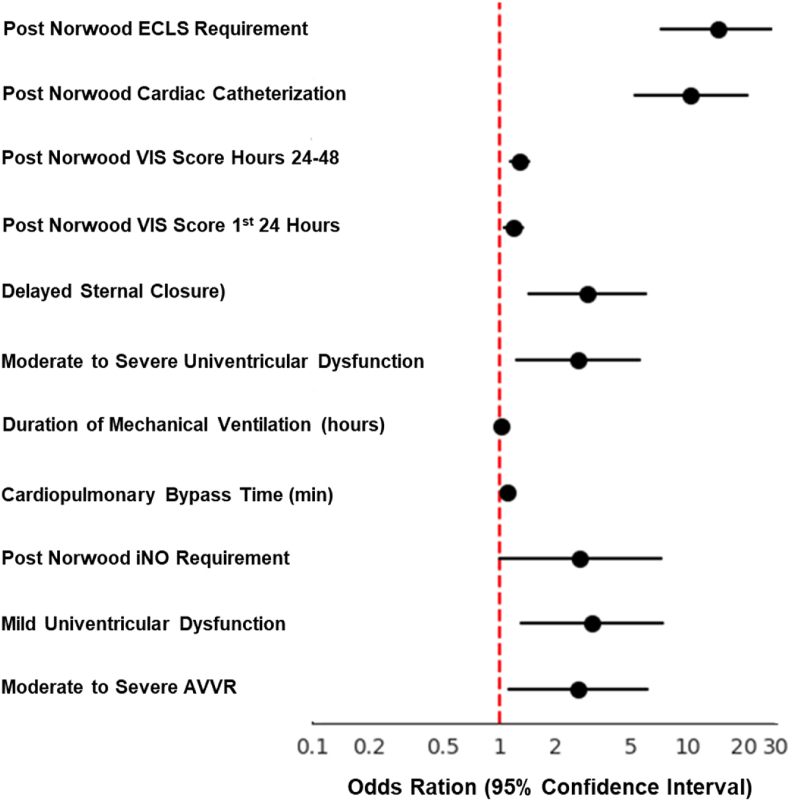
Of 269 patients undergoing NO, 213 (79.2 %) survived to discharge. Non-survivors had longer bypass times, delayed sternal closure, required nitric oxide, higher vasoactive scores, required post-operative catheterization, Extracorporeal Life Support (ECLS), and longer ventilation (p < 0.05). Logistic regression showed moderate-severe atrioventricular valve regurgitation on intraoperative TEE (OR 2.6), requiring nitric oxide (OR 2.63), delayed sternal closure (OR 2.94), post-operative catheterization (OR 10.48), and ECLS (OR 14.54) increased mortality odds (p < 0.05). Multivariable analysis confirmed catheterization (aOR 10.48) and ECLS (aOR 14.54) as significant predictors. Of survivors, 26 (12.3 %) developed new morbidity, 9 (4.2 %) had unfavorable outcomes. Functional status improved from 6.0 to 8.04, mainly in feeding and respiratory domains (p < 0.0001).
Norwood survival was 79.2 %. Requiring post-operative catheterization and ECLS significantly increased mortality risk. Multicenter evaluation of these modifiable risk factors is needed to improve outcomes in this high-risk population.
用于单心室生理患儿的诺伍德手术(NO)术间死亡率很高。本研究评估了诺伍德手术后的结局及死亡风险因素。
对2010年至2020年接受诺伍德手术的患者进行回顾性单中心研究。分析采用了适当的统计学方法。
在269例接受诺伍德手术的患者中,213例(79.2%)存活至出院。未存活者体外循环时间更长、胸骨闭合延迟、需要一氧化氮、血管活性评分更高、术后需要导管插入术、体外膜肺氧合(ECLS)以及机械通气时间更长(p<0.05)。逻辑回归显示,术中经食管超声心动图(TEE)提示中重度房室瓣反流(比值比[OR]为2.6)、需要一氧化氮(OR为2.63)、胸骨闭合延迟(OR为2.94)、术后导管插入术(OR为10.48)以及ECLS(OR为14.54)会增加死亡几率(p<0.05)。多变量分析证实导管插入术(校正OR为10.48)和ECLS(校正OR为14.54)是显著的预测因素。在存活者中,26例(12.3%)出现了新的并发症,9例(4.2%)预后不佳。功能状态从6.0改善至8.04,主要在喂养和呼吸领域(p<0.0001)。
诺伍德手术的存活率为79.2%。术后需要导管插入术和ECLS会显著增加死亡风险。需要对这些可改变的风险因素进行多中心评估,以改善这一高危人群的结局。