Wang Jiuyi, Wang Kai, Feng Guibo, Tian Xin
Department of General Medicine, Yongchuan Hospital of Chongqing Medical University, Chongqing 402160, China.
Department of Cardiology, The Second Affiliated Hospital of Chongqing Medical University, Chongqing 401336, China.
Glob Heart. 2024 Dec 19;19(1):97. doi: 10.5334/gh.1379. eCollection 2024.
The albumin-bilirubin (ALBI) score has demonstrated prognostic value in a range for liver and heart diseases. However, its association with all-cause mortality in intensive care unit (ICU) patients with heart failure remains uncertain.
This study sought to investigate the relationship between the ALBI score and the risk of all-cause mortality in ICU patients with heart failure.
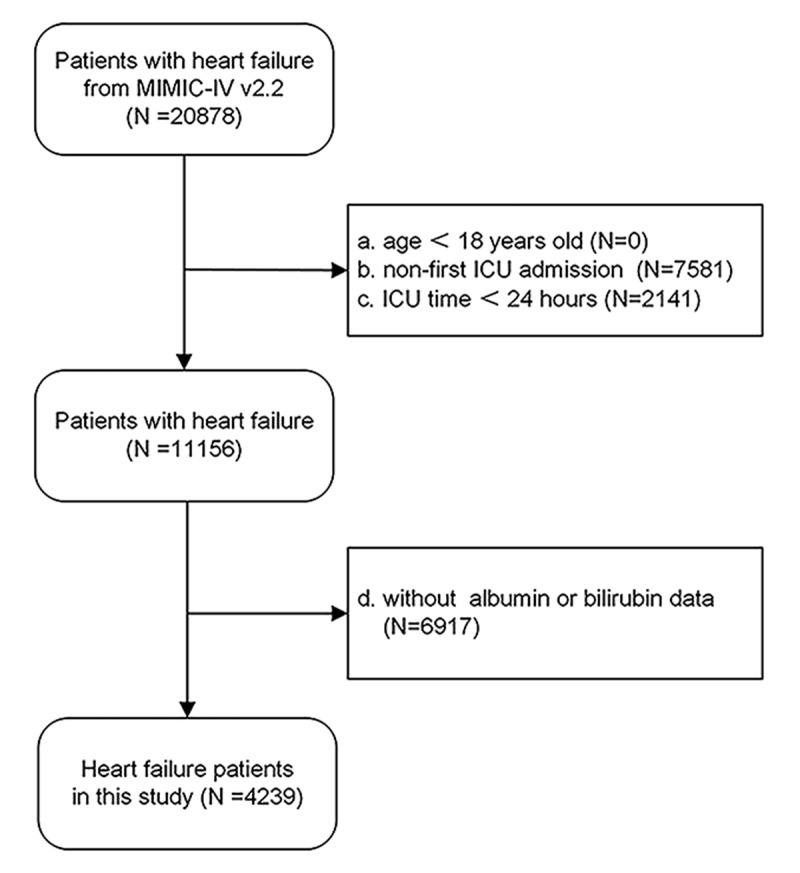
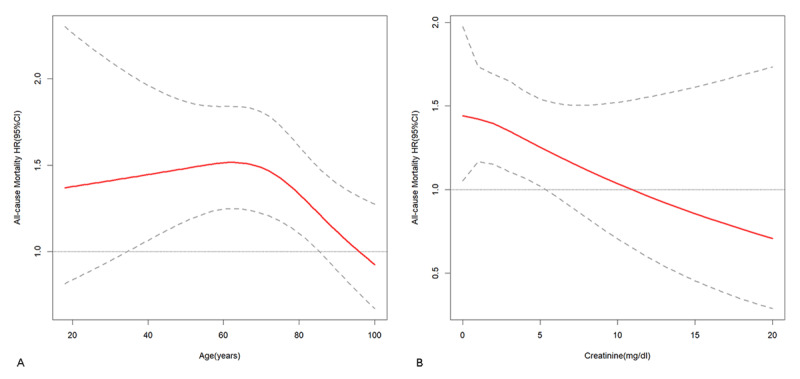
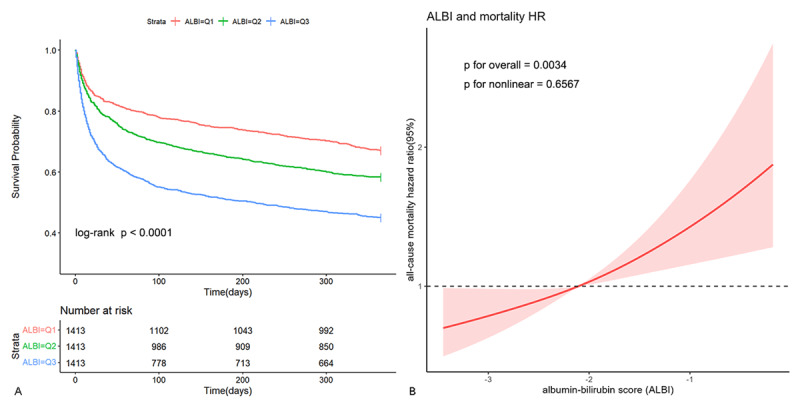
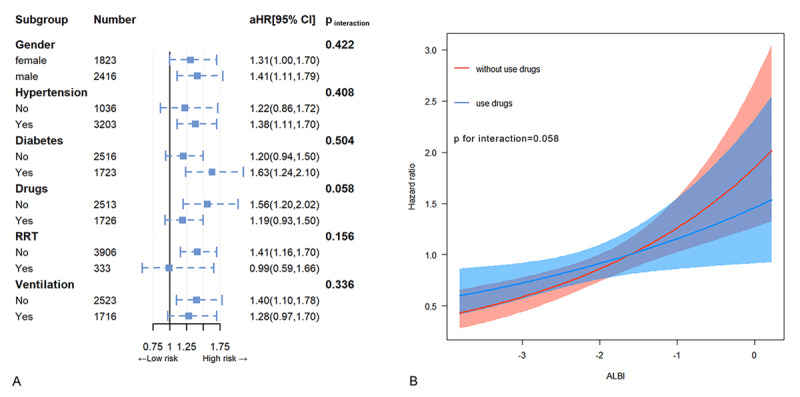
The ICU patients diagnosed with heart failure were selected from the Medical Information Mart for Intensive Care IV database (MIMIC-IV, version 2.2) and stratified into tertiles according to their ALBI scores. The primary outcome of interest was the occurrence of all-cause mortality within 365 days post-discharge. The analysis encompassed a cohort of 4,239 patients, with Kaplan-Meier curves indicating that individuals with higher ALBI levels exhibited an elevated risk of all-cause mortality (log-rank p < 0.001). Multivariate adjusted Cox regression and subgroup analysis demonstrated that individuals in T2 (hazard ratio (HR) 1.09, 95% CI 0.99-1.21) and T3 (HR 1.17, 95% CI 1.02-1.34) had an increased risk of mortality compared to individuals in T1 (p for trend < 0.001), and each incremental tertile in ALBI was linked to a 10% rise in mortality risk, while each individual unit increase in ALBI was associated with a 36% increase in mortality risk. This relationship was consistently observed across most subgroups, except for using or not using inotropes or vasopressors, different ages, different creatinine levels. The restricted cubic spline (RCS) analysis indicated a linear relationship between ALBI levels and the risk of all-cause mortality.
The ALBI scores are independently associated with the risk of all-cause mortality in ICU patients with heart failure, particularly in those not using inotropes or vasopressors, younger patients, and with lower levels of creatinine. ALBI may help identify high-risk patients and optimize risk stratification in this population.
白蛋白-胆红素(ALBI)评分已在一系列肝脏和心脏疾病中显示出预后价值。然而,其与重症监护病房(ICU)心力衰竭患者全因死亡率的关联仍不确定。
本研究旨在探讨ALBI评分与ICU心力衰竭患者全因死亡风险之间的关系。
从重症监护医学信息数据库IV(MIMIC-IV,版本2.2)中选取诊断为心力衰竭的ICU患者,并根据其ALBI评分分为三分位数。感兴趣的主要结局是出院后365天内全因死亡的发生情况。该分析纳入了4239例患者的队列,Kaplan-Meier曲线表明,ALBI水平较高的个体全因死亡风险升高(对数秩p<0.001)。多变量调整后的Cox回归和亚组分析表明,与T1组个体相比,T2组(风险比(HR)1.09,95%置信区间0.99-1.21)和T3组(HR 1.17,95%置信区间1.02-1.34)的个体死亡风险增加(趋势p<0.001),ALBI每增加一个三分位数与死亡风险增加10%相关,而ALBI每增加一个单位与死亡风险增加36%相关。除了是否使用血管活性药物、不同年龄、不同肌酐水平外,在大多数亚组中均观察到这种关系。受限立方样条(RCS)分析表明ALBI水平与全因死亡风险之间存在线性关系。
ALBI评分与ICU心力衰竭患者的全因死亡风险独立相关,尤其是在未使用血管活性药物的患者、年轻患者以及肌酐水平较低的患者中。ALBI可能有助于识别该人群中的高危患者并优化风险分层。