Tain You-Lin, Li Lung-Chih, Kuo Hsiao-Ching, Chen Chiu-Ju, Hsu Chien-Ning
Department of Pediatrics, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
Institute for Translational Research in Biomedicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
JAMA Pediatr. 2025 Feb 1;179(2):171-178. doi: 10.1001/jamapediatrics.2024.4409.
Gestational exposure to nonsteroidal anti-inflammatory drugs (NSAIDs) may increase the risk of adverse fetal kidney outcomes. However, details regarding timing, specific NSAIDs, and long-term childhood kidney outcomes are limited.
To evaluate the association between gestational exposure to NSAIDs and the risk of chronic kidney disease (CKD) in childhood.
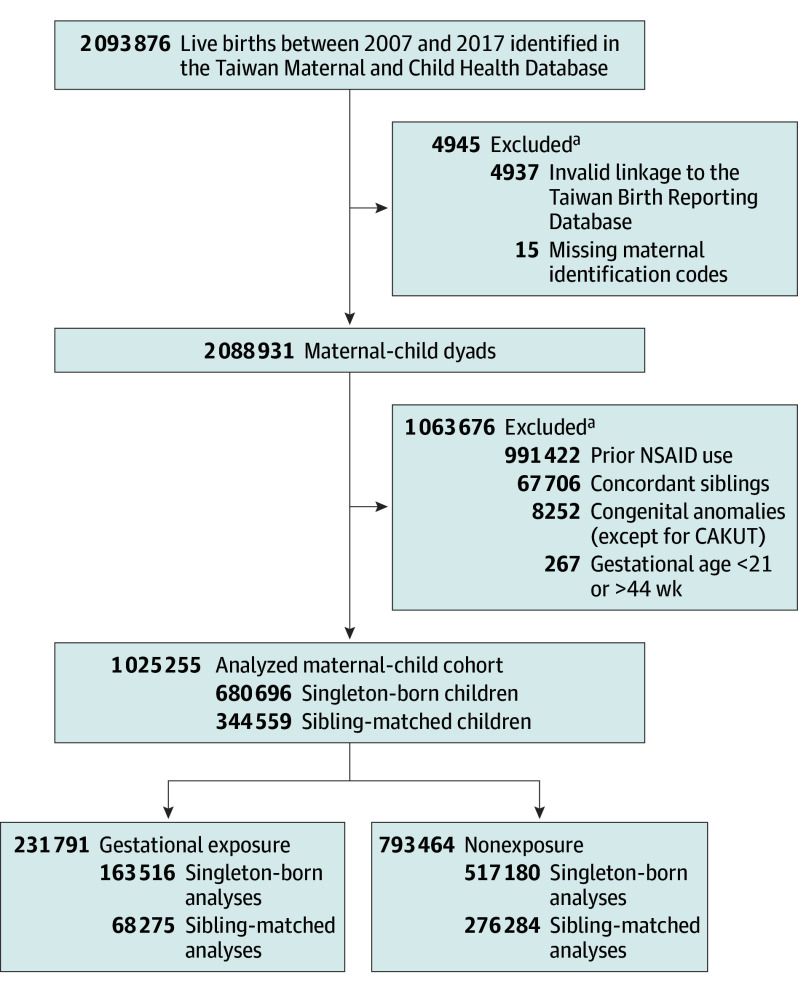
DESIGN, SETTING, AND PARTICIPANTS: This national cohort study assessed 1 025 255 children born alive in Taiwan from January 1, 2007, to December 31, 2017, with follow-up until December 31, 2021. Children without valid maternal-child linkage and with incomplete birth information were excluded. Data analysis was performed from November 30, 2023, to April 30, 2024.
Maternal prescriptions for NSAIDs from the last menstrual period to birth.
The main outcome was childhood CKD, including congenital anomalies of the kidney and urinary tract and other kidney diseases. Cox proportional hazards regression models with stabilized inverse probability of treatment weighting (weighted hazard ratio [wHR]) and a robust sandwich estimator were used to estimate the relative risk of NSAID exposure in pregnancy, adjusted for newborn characteristics.
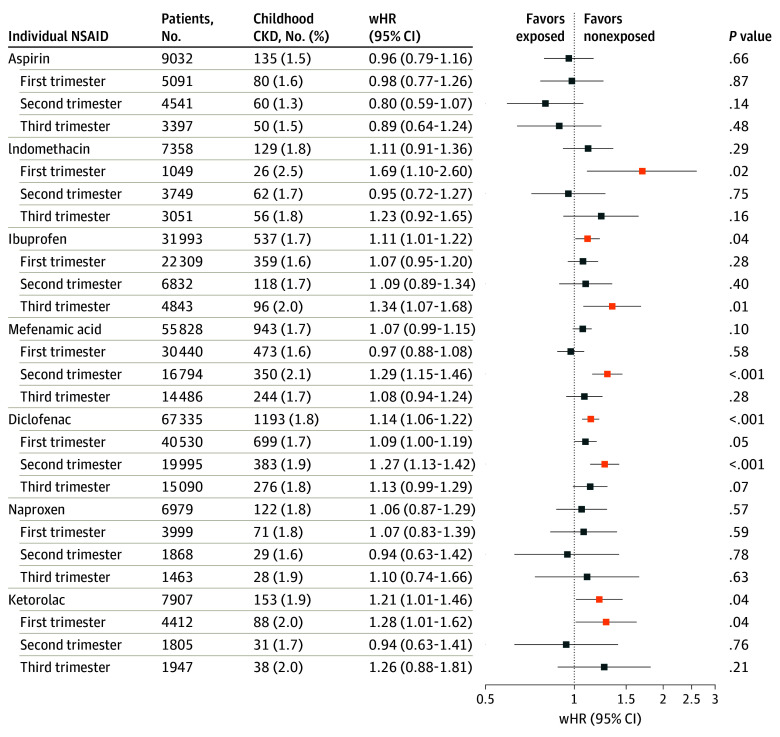
This study included 163 516 singleton-born children (24.0%) whose mothers (mean [SD] age at birth of child, 31.25 [4.92] years) used at least 1 dispensing of an NSAID during pregnancy. Gestational NSAID exposure was significantly associated with a higher risk of childhood CKD (wHR, 1.10; 95% CI, 1.05-1.15). No association was observed between NSAID use and fetal nephrotoxicity in sibling comparisons. Elevated risks were revealed for exposure during the second trimester (wHR, 1.19; 95% CI, 1.11-1.28) and the third trimester (wHR, 1.12; 95% CI, 1.03-1.22) in singleton-born children. Specific NSAID exposures associated with higher CKD risk included indomethacin (wHR, 1.69; 95% CI, 1.10-2.60) and ketorolac (wHR, 1.28; 95% CI, 1.01-1.62) in the first trimester, diclofenac (wHR, 1.27; 95% CI, 1.13-1.42) and mefenamic acid (wHR, 1.29; 95% CI, 1.15-1.46) in the second trimester, and ibuprofen (wHR, 1.34; 95% CI, 1.07-1.68) in the third trimester.
In this study, gestational exposure to NSAIDs was not associated with a substantial increase in the risk of childhood CKD when comparing between siblings. However, the findings underscore the need for caution when prescribing NSAIDs during pregnancy, particularly indomethacin and ketorolac in the first trimester, mefenamic acid and diclofenac in the second trimester, and ibuprofen in the third trimester, to ensure the safety of the offspring's kidneys.
孕期接触非甾体抗炎药(NSAIDs)可能会增加胎儿出现不良肾脏结局的风险。然而,关于接触时间、具体的非甾体抗炎药以及儿童期长期肾脏结局的详细信息有限。
评估孕期接触非甾体抗炎药与儿童慢性肾脏病(CKD)风险之间的关联。
设计、背景和参与者:这项全国性队列研究评估了2007年1月1日至2017年12月31日在台湾地区出生的1025255名活产儿童,随访至2021年12月31日。排除了母婴关联无效以及出生信息不完整的儿童。数据分析于2023年11月30日至2024年4月30日进行。
从末次月经到分娩期间母亲开具的非甾体抗炎药处方。
主要结局是儿童慢性肾脏病,包括先天性肾脏和尿路异常以及其他肾脏疾病。采用带有稳定化治疗权重逆概率的Cox比例风险回归模型(加权风险比[wHR])和稳健的三明治估计量来估计孕期接触非甾体抗炎药的相对风险,并根据新生儿特征进行调整。
本研究纳入了163516名单胎出生儿童(占24.0%),其母亲(孩子出生时的平均[标准差]年龄为31.25[4.92]岁)在孕期至少使用过1次非甾体抗炎药。孕期接触非甾体抗炎药与儿童慢性肾脏病风险显著升高相关(wHR,1.10;95%置信区间,1.05 - 1.15)。在同胞比较中,未观察到非甾体抗炎药使用与胎儿肾毒性之间的关联。单胎出生儿童在孕中期(wHR,1.19;95%置信区间,1.11 - 1.28)和孕晚期(wHR,1.12;95%置信区间,1.03 - 1.22)接触非甾体抗炎药的风险升高。与慢性肾脏病风险较高相关的特定非甾体抗炎药暴露包括孕早期的吲哚美辛(wHR,1.69;95%置信区间,1.10 - 2.60)和酮咯酸(wHR,1.28;95%置信区间,1.01 - 1.62),孕中期的双氯芬酸(wHR,1.27;95%置信区间,1.13 - 1.42)和甲芬那酸(wHR,1.29;95%置信区间,1.15 - 1.46),以及孕晚期的布洛芬(wHR,1.34;95%置信区间,1.07 - 1.68)。
在本研究中,同胞间比较时,孕期接触非甾体抗炎药与儿童慢性肾脏病风险的大幅增加无关。然而,研究结果强调了孕期开具非甾体抗炎药时需谨慎,尤其是孕早期的吲哚美辛和酮咯酸、孕中期的甲芬那酸和双氯芬酸以及孕晚期的布洛芬,以确保后代肾脏的安全。