Lukwaro Andrew, Lu Yi, Chen Junzhe, Tang Ying
Department of Nephrology, Third Affiliated Hospital of Southern Medical University, Guangzhou, China.
BMC Nephrol. 2024 Dec 23;25(1):471. doi: 10.1186/s12882-024-03872-9.
Contrast-induced acute kidney injury (CI-AKI) is a known complication after coronary angiography (CAG) or percutaneous coronary intervention (PCI). Clinical evidence suggests that trimetazidine (TMZ), an anti-ischemic drug, may prevent CI-AKI. We aimed to evaluate the role of trimetazidine in preventing CI-AKI in patients with pre-existing renal dysfunction undergoing CAG or PCI.
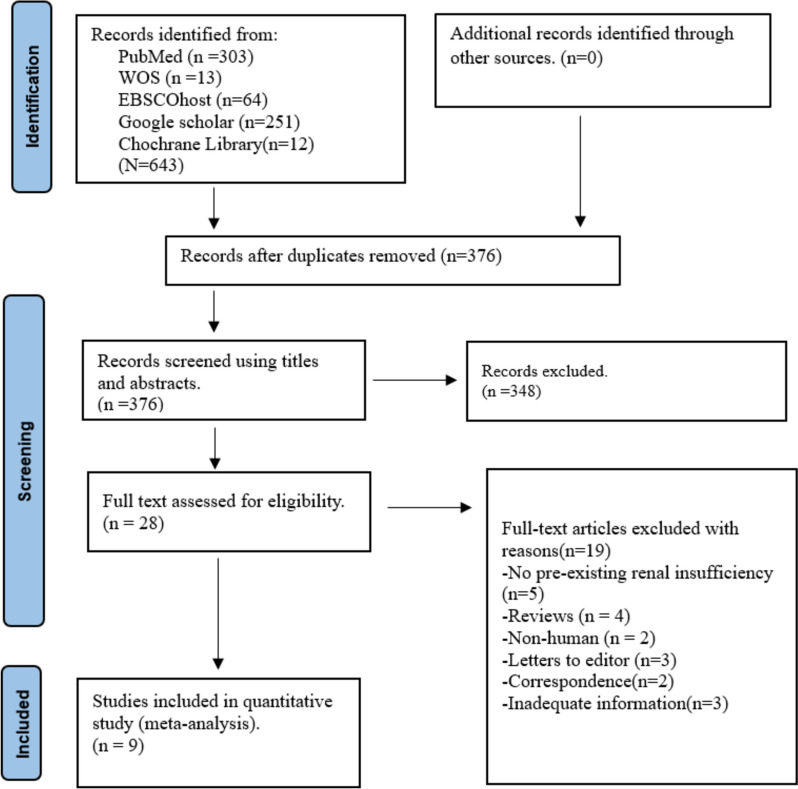
We searched PubMed, Cochrane Library, EBSCOhost, Web of Science, and Google Scholar databases from January 2004 to January 2024. We reviewed RCTs involving participants aged ≥ 18 years with pre-existing renal insufficiency who underwent CAG or PCI. Outcomes should include the incidence of CI-AKI, adverse events, and changes in serum creatinine (Scr) levels at different time intervals. Two reviewers independently extracted the data, evaluated the quality and relevance of the studies, and graded the strength of evidence for each study through consensus.
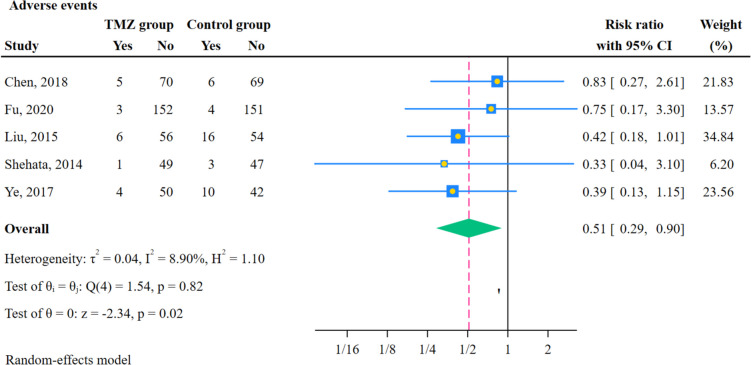
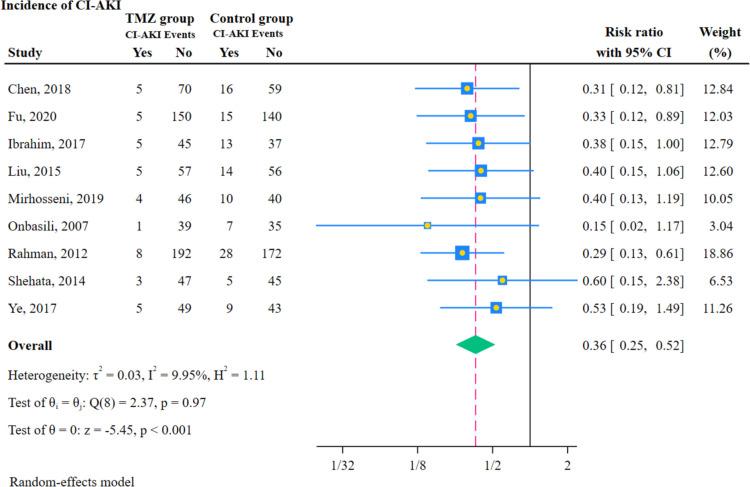
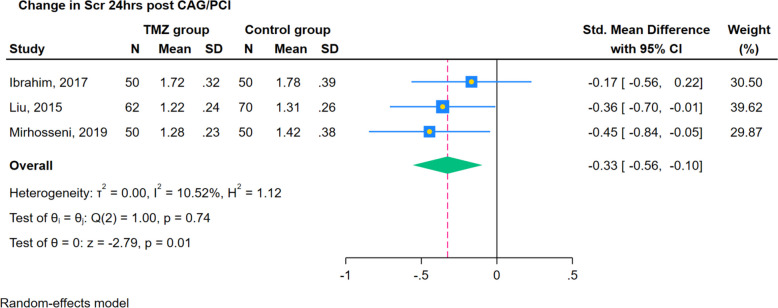
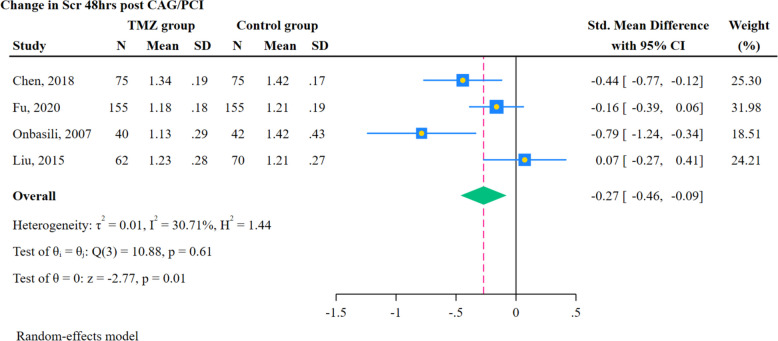
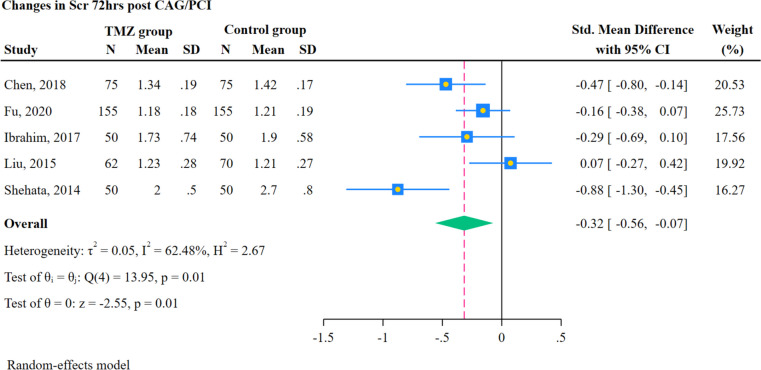
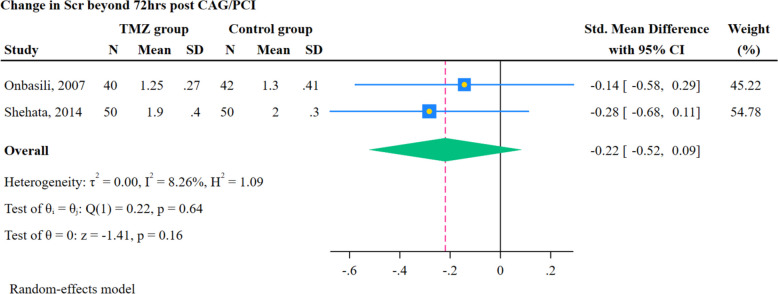
Nine RCTs met the inclusion criteria and assessed the role of TMZ in patients with renal dysfunction who underwent CAG or PCI. All RCTs showed a significant decrease in the incidence of CI-AKI in the TMZ group compared to the control group (RR 0.36, 95% CI, [0.25, 0.52] P < 0.001). Changes in Scr at 24 h (SMD -0.33, 95% CI, [-0.56, -0.10], P = 0.01), at 48 h (SMD -0.27, 95% CI, [-0.46, -0.09], P = 0.01), and 72 h (SMD -0.32, 95% CI, [-0.56, -0.07], P = 0.01) were statistically significant in the TMZ group compared to the control group. However, the changes in Scr beyond 72 h following CAG or PCI were statistically insignificant in the TMZ group when compared to the control group (SMD -0.22, 95% CI, [-0.52, 0.09], P = 0.16). The incidence of adverse effects was lower in the TMZ group than in the control group, and the difference was statistically significant (RR 0.51, 95% CI, [0.29, 0.90]; P = 0.02).
The addition of TMZ to standard hydration protocols may offer a promising strategy for lowering the incidence of CI-AKI, adverse events, and postoperative SCr levels in patients with renal insufficiency within 72 h after CAG or PCI. However, large-scale RCTs are necessary to definitively establish the efficacy and safety of TMZ in patients with renal insufficiency after CAG or PCI.
造影剂诱发的急性肾损伤(CI-AKI)是冠状动脉造影(CAG)或经皮冠状动脉介入治疗(PCI)后已知的并发症。临床证据表明,抗缺血药物曲美他嗪(TMZ)可能预防CI-AKI。我们旨在评估曲美他嗪在接受CAG或PCI的已有肾功能不全患者中预防CI-AKI的作用。
我们检索了2004年1月至2024年1月的 PubMed、Cochrane图书馆、EBSCOhost、Web of Science和谷歌学术数据库。我们回顾了涉及年龄≥18岁、已有肾功能不全且接受CAG或PCI的参与者的随机对照试验(RCT)。结局应包括CI-AKI的发生率、不良事件以及不同时间间隔血清肌酐(Scr)水平的变化。两名研究者独立提取数据,评估研究的质量和相关性,并通过共识对每项研究的证据强度进行分级。
9项RCT符合纳入标准,并评估了TMZ在接受CAG或PCI的肾功能不全患者中的作用。与对照组相比,所有RCT均显示TMZ组CI-AKI的发生率显著降低(风险比0.36,95%置信区间[0.25, 0.52],P < 0.001)。与对照组相比,TMZ组在24小时(标准化均数差-0.33,95%置信区间[-0.56, -0.10],P = 0.01)、48小时(标准化均数差-0.27,95%置信区间[-0.46, -0.09],P = 0.01)和72小时(标准化均数差-0.32,95%置信区间[-0.56, -0.07],P = 0.01)时Scr的变化具有统计学意义。然而,与对照组相比,CAG或PCI后72小时以上TMZ组Scr的变化无统计学意义(标准化均数差-0.22,95%置信区间[-0.52, 0.09],P = 0.16)。TMZ组不良反应的发生率低于对照组,差异具有统计学意义(风险比0.51,95%置信区间[0.29, 0.90];P = 0.02)。
在标准水化方案中添加TMZ可能为降低CAG或PCI后72小时内肾功能不全患者CI-AKI的发生率、不良事件及术后Scr水平提供一种有前景的策略。然而,需要大规模RCT来明确确立TMZ在CAG或PCI后肾功能不全患者中的疗效和安全性。