Gurevich-Shapiro Anna, Orbach-Zinger Sharon, Leader Avi, Stemer Galia, Wiznitzer Arnon, Singer Pierre, Davidovits Miriam, Shapiro Michael, Hamulyák Eva N, Raanani Pia, Spectre Galia
Department of Systems Immunology, Weizmann Institute of Science, Rehovot, Israel.
Division of Hematology, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel.
Res Pract Thromb Haemost. 2024 Oct 3;8(8):102579. doi: 10.1016/j.rpth.2024.102579. eCollection 2024 Nov.
Postpartum hemorrhage is considered a risk factor for pregnancy-associated complement-mediated hemolytic uremic syndrome (CM-HUS; previously known as atypical hemolytic uremic syndrome) but has not been systematically studied.
To systematically examine the role of postpartum hemorrhage in precipitating CM-HUS and to describe the characteristics of postpartum hemorrhage-associated CM-HUS, its prognosis and recommended management.
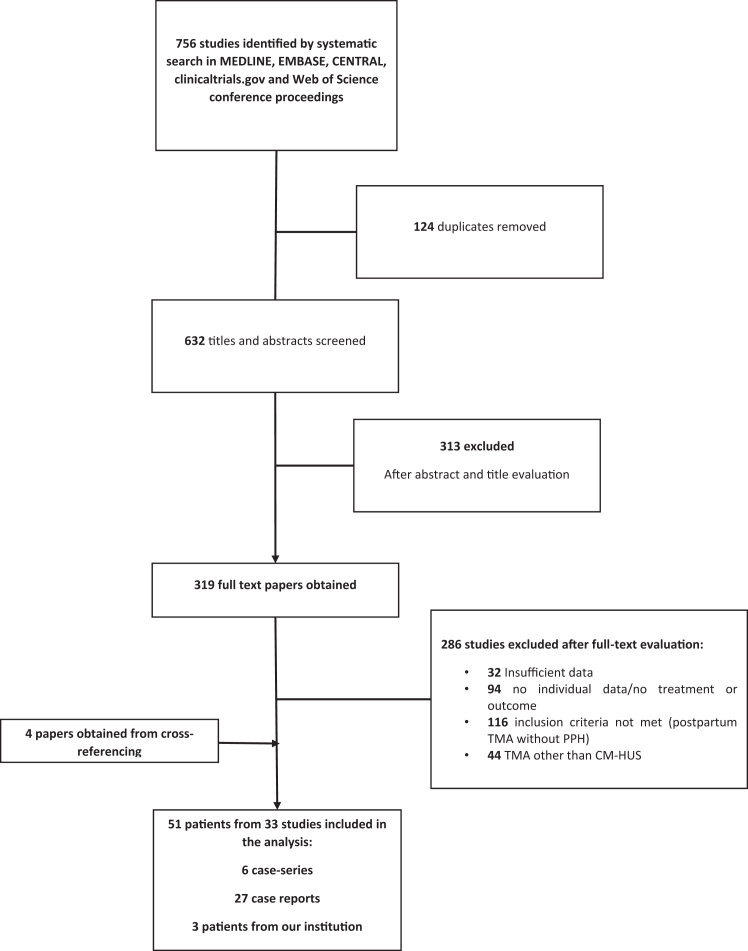
A systematic review of individual participant data from case series and reports in addition to a case series from our institution. Search terms were "thrombotic microangiopathy," "atypical hemolytic uremic syndrome," and "complement mediated" combined with "pregnancy," "postpartum," and/or "postpartum hemorrhage". Cases of thrombotic microangiopathy other than CM-HUS were excluded. Outcomes were clinical and laboratory characteristics of postpartum hemorrhage-associated CM-HUS, treatment, and outcomes.
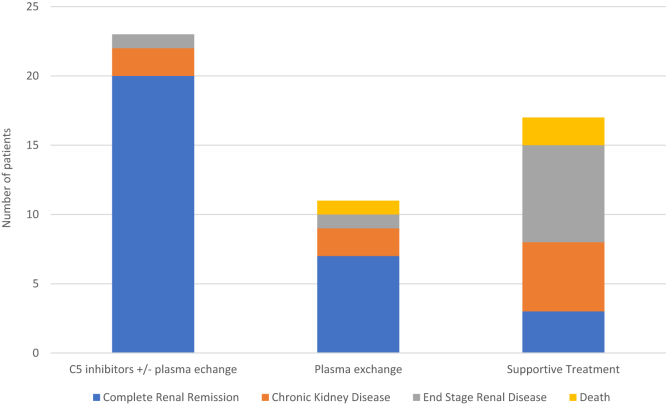
Thirty-three studies comprising 48 women with postpartum hemorrhage-associated CM-HUS and 3 patients from our institution were included in the study. Most women presented at term (28/45; 62%), delivered by cesarean section (21/41; 51%), and had pregnancy complications, mainly preeclampsia (16/51; 31%) or fetal demise (9/51; 18%). Hematological and renal abnormalities usually appeared within the first 24 hours postdelivery. The median platelet count was 46 × 10/L (IQR, 26-72), and the median maximal lactate dehydrogenase was 2638 U/L (IQR, 1620-3588). Renal function normalized in 20/23 (87%) women treated with C5 inhibitors with or without plasma exchange; in 7/11 (63%) women treated with plasma exchange alone, but only in 3/17 (18%) patients treated with supportive care. Patients treated with C5 inhibitors and/or plasma exchange achieved significantly better renal outcomes compared with supportive care alone ( < .001).
CM-HUS is a rare complication following postpartum hemorrhage and occurs mainly in women with preeclampsia and/or following cesarean section. Patients treated with C5 inhibitors and/or plasma exchange had a better renal prognosis compared with patients who received supportive treatment alone.
产后出血被认为是妊娠相关补体介导的溶血尿毒综合征(CM-HUS,以前称为非典型溶血尿毒综合征)的一个危险因素,但尚未得到系统研究。
系统研究产后出血在引发CM-HUS中的作用,并描述产后出血相关CM-HUS的特征、预后及推荐的治疗方法。
除了对我们机构的一个病例系列进行系统回顾外,还对来自病例系列和报告的个体参与者数据进行了系统回顾。检索词为“血栓性微血管病”“非典型溶血尿毒综合征”和“补体介导”,并与“妊娠”“产后”和/或“产后出血”相结合。排除CM-HUS以外的血栓性微血管病病例。结局指标为产后出血相关CM-HUS的临床和实验室特征、治疗及结局。
该研究纳入了33项研究,包括48例产后出血相关CM-HUS的女性和我们机构的3例患者。大多数女性为足月分娩(28/45;62%),通过剖宫产分娩(21/41;51%),并有妊娠并发症,主要是子痫前期(16/51;31%)或胎儿死亡(9/51;18%)。血液学和肾脏异常通常在产后24小时内出现。血小板计数中位数为46×10⁹/L(四分位间距,26-72),最大乳酸脱氢酶中位数为2638 U/L(四分位间距,1620-3588)。在接受C5抑制剂治疗(有或无血浆置换)的20/23(87%)女性中,肾功能恢复正常;在仅接受血浆置换治疗的7/11(63%)女性中,肾功能恢复正常,但在仅接受支持治疗的17/3(18%)患者中,肾功能恢复正常。与仅接受支持治疗相比,接受C5抑制剂和/或血浆置换治疗的患者肾脏结局明显更好(P<0.001)。
CM-HUS是产后出血后一种罕见的并发症,主要发生在子痫前期女性和/或剖宫产术后。与仅接受支持治疗的患者相比,接受C5抑制剂和/或血浆置换治疗的患者肾脏预后更好。