Zhu Ting, Mu Di, Hu Yao, Cao Yang, Yuan Minlan, Xu Jia, Ye Heng-Qing, Zhang Wei
West China Biomedical Big Data Center, West China Hospital, Sichuan University, Chengdu, 610041, China.
Med-X Center for Informatics, Sichuan University, Chengdu, 610041, China.
Transl Psychiatry. 2024 Dec 24;14(1):504. doi: 10.1038/s41398-024-03213-2.
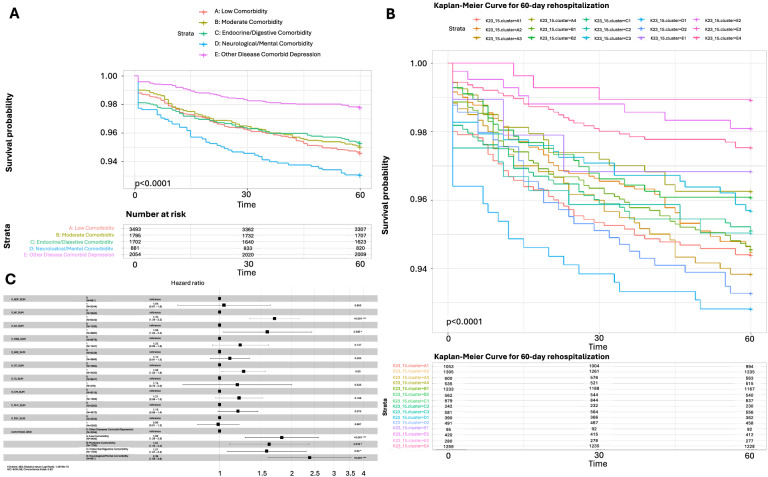
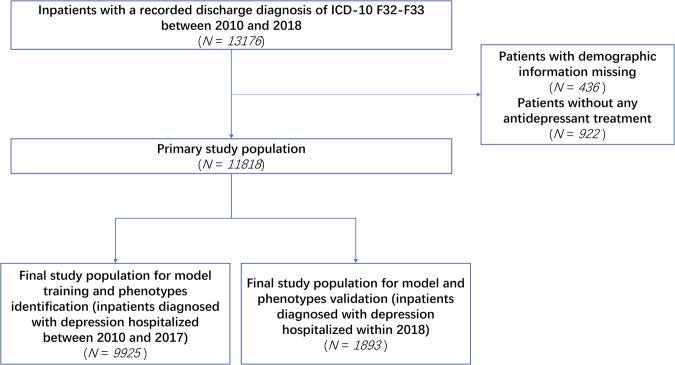
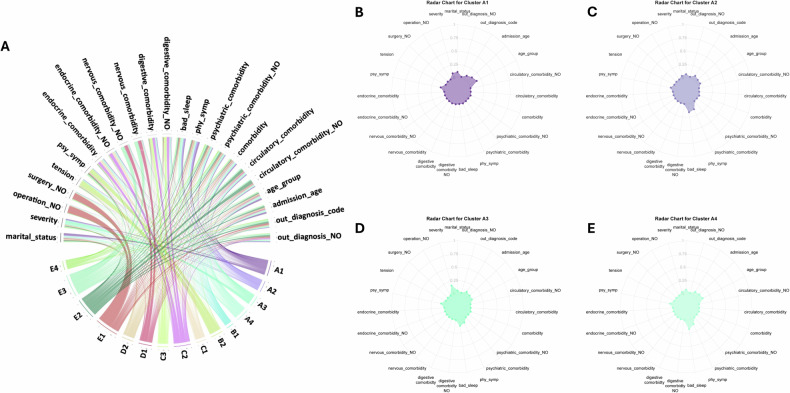
Depression is a heterogeneous and complex psychological syndrome with highly variable manifestations, which poses difficulties for treatment and prognosis. Depression patients are prone to developing various comorbidities, which stem from different pathophysiological mechanisms, remaining largely understudied. The current study focused on identifying comorbidity-specific phenotypes, and whether these clustered phenotypes are associated with different treatment patterns, clinical manifestations, physiological characteristics, and prognosis. We have conducted a 10-year retrospective observational cohort study using electronic medical records (EMR) for 11,818 patients diagnosed with depression and hospitalized at a large academic medical center in Chengdu, China. K-means clustering and visualization methods were performed to identify phenotypic categories. The association between phenotypic categories and clinical outcomes was evaluated using adjusted Cox proportional hazards model. We classified patients with depression into five stable phenotypic categories, including 15 statistically driven clusters in the discovery cohort (n = 9925) and the validation cohort (n = 1893), respectively. The categories include: (Category A) the lowest incidence of comorbidity, with prominent suicide, psychotic, and somatic symptoms (n = 3493/9925); (Category B) moderate comorbidity rate, with prominent anhedonia and anxious symptoms (n = 1795/9925); (Category C) the highest incidence of comorbidity of endocrine/metabolic and digestive system diseases (n = 1702/9925); (Category D) the highest incidence of comorbidity of neurological, mental and behavioral diseases (n = 881/9925); (Category E) other diseases comorbid with depression (n = 2054/9925). Patients in Category E had the lowest risk of psychiatric rehospitalization within 60-day follow-up, followed by Category C (HR, 1.57; 95% CI, 1.07-2.30), Category B (HR, 1.61; 95% CI, 1.10-2.40), Category A (HR, 1.82; 95% CI, 1.28-2.60), and Category D (HR, 2.38; 95% CI, 1.59-3.60) with P < 0.05, after adjustment for comorbidities, medications, and age. Regarding other longer observation windows (90-day, 180-day and 365-day), patients in Category D showed the highest rehospitalization risk all the time while there were notable shifts in rankings observed for Categories A, B and C over time. The results indicate that the higher the severity of mental illness in patients with five phenotypic categories, the greater the risk of rehospitalization. These phenotypes are associated with various pathways, including the cardiometabolic system, chronic inflammation, digestive system, neurological system, and mental and behavioral disorders. These pathways play a crucial role in connecting depression with other psychiatric and somatic diseases. The identified phenotypes exhibit notable distinctions in terms of comorbidity patterns, symptomology, biological characteristics, treatment approaches, and clinical outcomes.
抑郁症是一种异质性且复杂的心理综合征,表现高度多变,这给治疗和预后带来困难。抑郁症患者容易并发多种疾病,这些疾病源于不同的病理生理机制,目前在很大程度上仍未得到充分研究。当前的研究聚焦于识别特定共病的表型,以及这些聚类表型是否与不同的治疗模式、临床表现、生理特征和预后相关。我们利用中国成都一家大型学术医疗中心的11818例诊断为抑郁症并住院的患者的电子病历(EMR)进行了一项为期10年的回顾性观察队列研究。采用K均值聚类和可视化方法来识别表型类别。使用调整后的Cox比例风险模型评估表型类别与临床结局之间的关联。我们将抑郁症患者分为五个稳定的表型类别,在发现队列(n = 9925)和验证队列(n = 1893)中分别包括15个由统计驱动的聚类。这些类别包括:(A类)共病发生率最低,有突出的自杀、精神病性和躯体症状(n = 3493/9925);(B类)共病率中等,有突出的快感缺失和焦虑症状(n = 1795/9925);(C类)内分泌/代谢和消化系统疾病共病发生率最高(n = 1702/9925);(D类)神经、精神和行为疾病共病发生率最高(n = 881/9925);(E类)与抑郁症共病的其他疾病(n = 2054/9925)。在60天随访期内,E类患者精神科再次住院风险最低,其次是C类(风险比[HR],1.57;95%置信区间[CI],1.07 - 2.30)、B类(HR,1.61;95% CI,1.10 - 2.40)、A类(HR,1.82;95% CI,1.28 - 2.60)和D类(HR,2.38;95% CI,1.59 - 3.60),P < 0.05,在对共病、用药和年龄进行调整后。关于其他更长的观察窗口(90天、180天和365天),D类患者始终显示出最高的再次住院风险,而随着时间推移,A类、B类和C类的排名有显著变化。结果表明,五个表型类别的患者精神疾病严重程度越高,再次住院风险越大。这些表型与多种途径相关,包括心脏代谢系统、慢性炎症、消化系统、神经系统以及精神和行为障碍。这些途径在将抑郁症与其他精神和躯体疾病联系起来方面起着关键作用。所识别出的表型在共病模式、症状学、生物学特征、治疗方法和临床结局方面表现出显著差异。