Division of Research, Kaiser Permanente Northern California, Oakland.
Kaiser Permanente Washington Health Research Institute, Kaiser Permanente Washington, Seattle.
JAMA Netw Open. 2020 Dec 1;3(12):e2029068. doi: 10.1001/jamanetworkopen.2020.29068.
Medically complex patients are a heterogeneous group that contribute to a substantial proportion of health care costs. Coordinated efforts to improve care and reduce costs for this patient population have had limited success to date.
To define distinct patient clinical profiles among the most medically complex patients through clinical interpretation of analytically derived patient clusters.
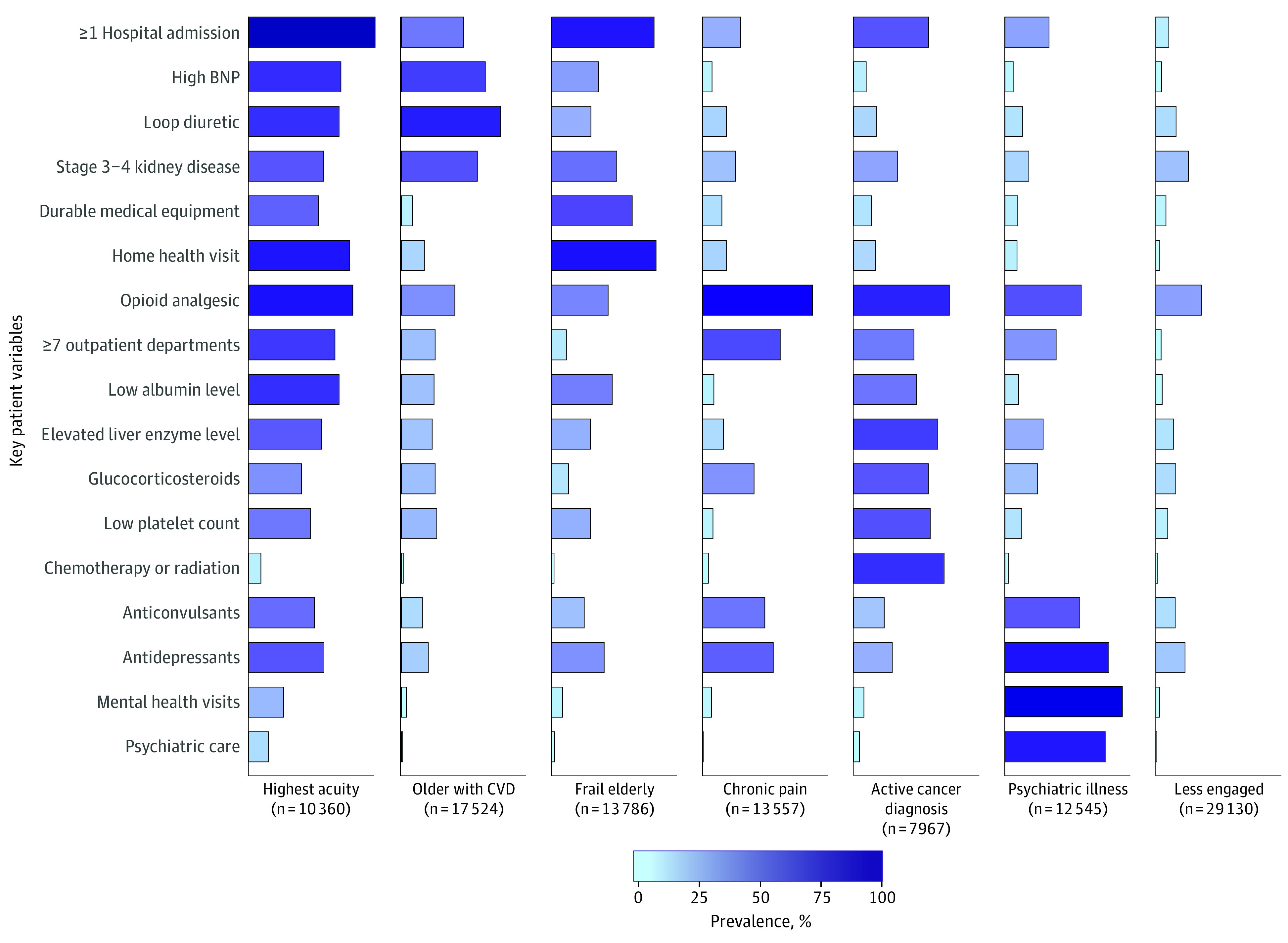
DESIGN, SETTING, AND PARTICIPANTS: This cohort study analyzed the most medically complex patients within Kaiser Permanente Northern California, a large integrated health care delivery system, based on comorbidity score, prior emergency department admissions, and predicted likelihood of hospitalization, from July 18, 2018, to July 15, 2019. From a starting point of over 5000 clinical variables, we used both clinical judgment and analytic methods to reduce to the 97 most informative covariates. Patients were then grouped using 2 methods (latent class analysis, generalized low-rank models, with k-means clustering). Results were interpreted by a panel of clinical stakeholders to define clinically meaningful patient profiles.
Complex patient profiles, 1-year health care utilization, and mortality outcomes by profile.
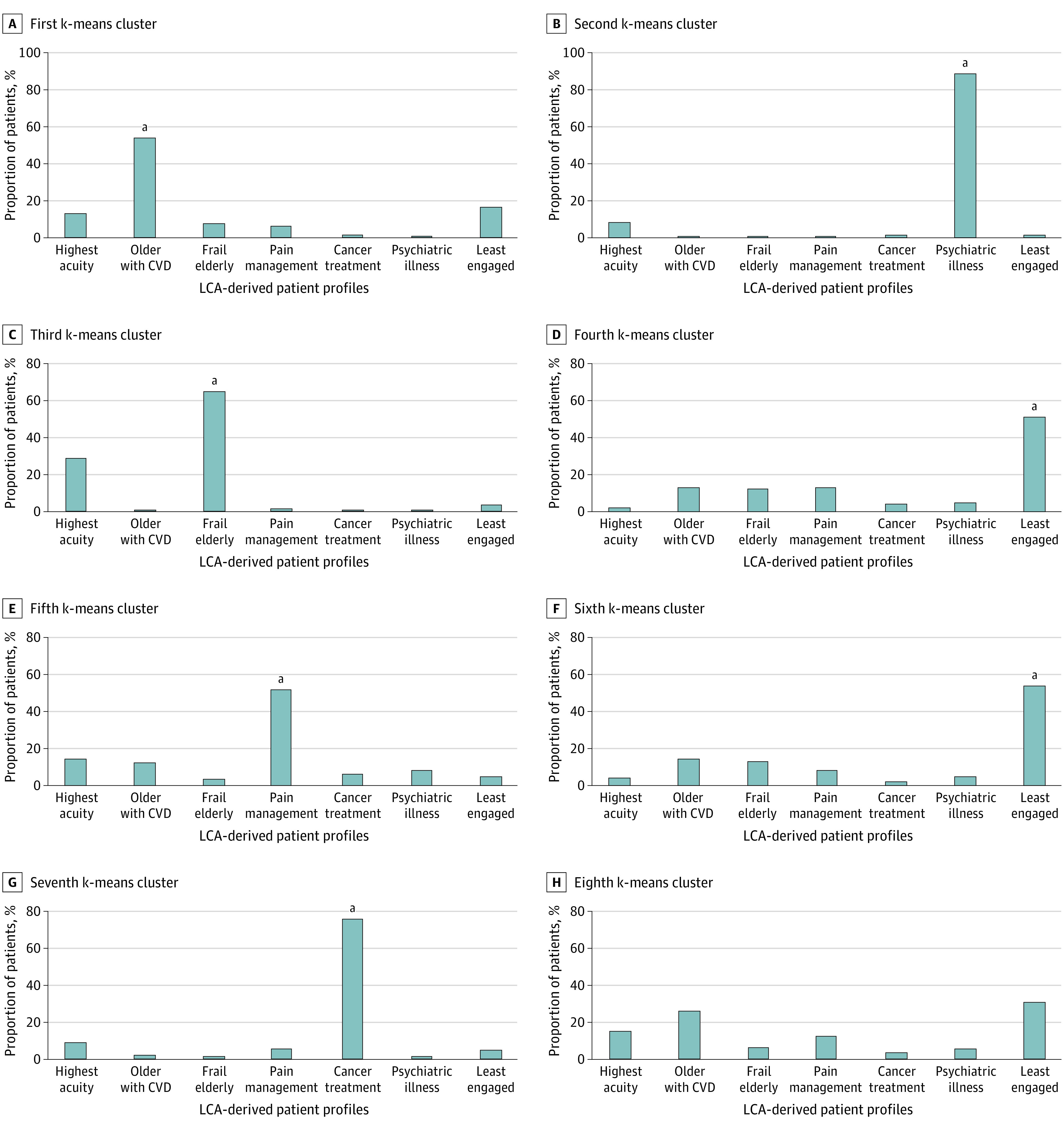
The analysis included 104 869 individuals representing 3.3% of the adult population (mean [SD] age, 70.7 [14.5] years; 52.4% women; 39% non-White race/ethnicity). Latent class analysis resulted in a 7-class solution. Stakeholders defined the following complex patient profiles (prevalence): high acuity (9.4%), older patients with cardiovascular complications (15.9%), frail elderly (12.5%), pain management (12.3%), psychiatric illness (12.0%), cancer treatment (7.6%), and less engaged (27%). Patients in these groups had significantly different 1-year mortality rates (ranging from 3.0% for psychiatric illness profile to 23.4% for frail elderly profile; risk ratio, 7.9 [95% CI, 7.1-8.8], P < .001). Repeating the analysis using k-means clustering resulted in qualitatively similar groupings. Each clinical profile suggested a distinct collaborative care strategy to optimize management.
The findings suggest that highly medically complex patient populations may be categorized into distinct patient profiles that are amenable to varying strategies for resource allocation and coordinated care interventions.
患有多种疾病的患者是一个异质群体,他们在医疗保健费用中占了相当大的比例。迄今为止,为改善这一患者群体的护理和降低成本而进行的协调努力收效甚微。
通过对分析得出的患者聚类进行临床解释,确定最具医疗复杂性患者中的不同患者临床特征。
设计、设置和参与者:这项队列研究分析了 Kaiser Permanente Northern California 内最具医疗复杂性的患者,这是一个大型综合医疗服务系统,其依据是合并症评分、先前的急诊就诊次数和预测的住院可能性,时间范围为 2018 年 7 月 18 日至 2019 年 7 月 15 日。从 5000 多个临床变量出发,我们使用临床判断和分析方法将其减少到 97 个最具信息量的协变量。然后,我们使用两种方法(潜在类别分析、广义低秩模型和 K 均值聚类)对患者进行分组。结果由一组临床利益相关者进行解释,以确定具有临床意义的患者特征。
复杂患者特征、1 年医疗保健利用率和按特征分类的死亡率结果。
该分析包括 104869 名代表成人人口 3.3%的个体(平均[SD]年龄为 70.7[14.5]岁;52.4%为女性;39%为非白种人/族裔)。潜在类别分析得出了 7 类解决方案。利益相关者定义了以下复杂的患者特征(患病率):高急症(9.4%)、心血管并发症老年患者(15.9%)、体弱老年患者(12.5%)、疼痛管理(12.3%)、精神疾病(12.0%)、癌症治疗(7.6%)和参与度低(27.0%)。这些组的患者 1 年死亡率有显著差异(范围从精神疾病特征的 3.0%到体弱老年患者的 23.4%;风险比为 7.9[95%CI,7.1-8.8],P < .001)。使用 K 均值聚类重复分析得到了定性上相似的分组。每个临床特征都提示了一种不同的协作护理策略,以优化管理。
研究结果表明,高度患有多种疾病的患者群体可能可以分为不同的患者特征,这些特征可以通过不同的资源分配策略和协调的护理干预措施来处理。