Ho Frederick K, Allan Max, Shao Hui, Man Kenneth K C, Jani Bhautesh D, Lyall Donald, Hastie Claire, Fleming Michael, Mackay Daniel, Cleland John G F, Delles Christian, Dundas Ruth, Lewsey Jim, Ip Patrick, Wong Ian, Welsh Paul, Pearce Anna, Wright Charlotte M, Minnis Helen, Katikireddi S Vittal, Pell Jill P
School of Health and Wellbeing, University of Glasgow, UK.
School of Pharmacy, University College London, UK.
Lancet Reg Health Eur. 2024 Oct 1;47:101075. doi: 10.1016/j.lanepe.2024.101075. eCollection 2024 Dec.
Socioeconomic inequality in infant mortality in the UK is rising. This study aims to identify contributory maternal and pregnancy factors that can explain the known association between area deprivation and infant mortality.
A cohort study was conducted using Clinical Practice Research Datalink (CPRD) primary care data between 2004 and 2019 linked to the Index of Multiple Deprivation (IMD), and infant mortality from the Office for National Statistics death data. Potential maternal and pregnancy contributory factors included: maternal age, prior maternal health conditions, pregnancy lifestyle factors and complications, use of medications during pregnancy, and characteristics of birth. Counterfactual-based decomposition analysis was used to quantify the relative importance of equalising these factors to reduce inequalities in infant mortality.
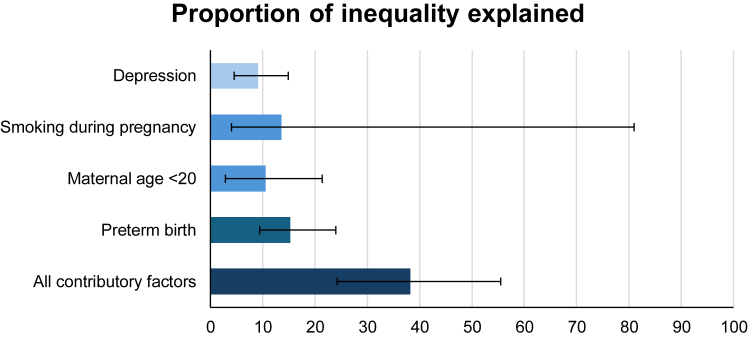
A total of 392,606 mother-child dyads were included in this study. The overall risk of infant mortality was greatest for individuals in the most deprived quintile (risk ratio 2.13 [95% CI 1.58-2.90]; risk difference 6.6 [3.8-8.8] per 10,000 live births) compared with the least deprived. Four contributory factors were identified as potentially important: preterm birth (Proportion eliminated [PE] 15.25% [95% CI 9.44-24.12%]), smoking during pregnancy (PE 13.61% [95% CI 3.96-80.97%]), maternal age <20 years at childbirth (PE 10.52% [95% CI 2.93-21.35%]) and maternal depression (PE 9.13% [95% CI 4.47-14.93%]). These collectively accounted for more than one-third of the socioeconomic inequality in mortality.
Multifactorial interventions targeting maternal mental health, smoking, teenage pregnancy and preterm birth may mitigate a proportion of the effects of socioeconomic inequality but targeting these, alone, will not stem the rise in infant mortality. Structural efforts to reduce socioeconomic inequalities will also be required to prevent these excess infant deaths.
UK Medical Research Council, Scottish Chief Scientist Office, Wellcome Trust.
英国婴儿死亡率的社会经济不平等现象正在加剧。本研究旨在确定有助于解释地区贫困与婴儿死亡率之间已知关联的孕产妇和孕期因素。
利用临床实践研究数据链(CPRD)2004年至2019年的初级保健数据,并将其与多重贫困指数(IMD)以及国家统计局死亡数据中的婴儿死亡率相链接,开展了一项队列研究。潜在的孕产妇和孕期促成因素包括:产妇年龄、既往孕产妇健康状况、孕期生活方式因素和并发症、孕期用药情况以及分娩特征。基于反事实的分解分析用于量化均衡这些因素对减少婴儿死亡率不平等的相对重要性。
本研究共纳入392,606对母婴。与最不贫困五分位人群相比,最贫困五分位人群的婴儿总体死亡风险最高(风险比2.13 [95%置信区间1.58 - 2.90];每10,000例活产的风险差异为6.6 [3.8 - 8.8])。确定了四个可能重要的促成因素:早产(消除比例[PE] 15.25% [95%置信区间9.44 - 24.12%])、孕期吸烟(PE 13.61% [95%置信区间3.96 - 80.97%])、分娩时产妇年龄<20岁(PE 10.52% [95%置信区间2.93 - 21.35%])以及产妇抑郁(PE 9.13% [95%置信区间4.47 - 14.93%])。这些因素共同占死亡率社会经济不平等的三分之一以上。
针对孕产妇心理健康、吸烟、青少年怀孕和早产的多因素干预措施可能会减轻社会经济不平等的部分影响,但仅针对这些因素并不能阻止婴儿死亡率的上升。还需要采取结构性措施来减少社会经济不平等,以防止这些额外的婴儿死亡。
英国医学研究理事会、苏格兰首席科学家办公室、惠康信托基金会。