Van Nechel Christian, Duquesne Ulla, Toupet Michel, Hautefort Charlotte
Dizzy-Care - Clinique des Vertiges, Brussels, Belgium.
Institut de Recherche Oto-Neurologique (IRON), Paris, France.
Front Neurol. 2024 Dec 12;15:1509762. doi: 10.3389/fneur.2024.1509762. eCollection 2024.
While most head movements in daily life are active, most tools used to assess vestibular deficits rely on passive head movements. A single gain value is not sufficient to quantify gaze stabilization efficiency during active movements in vestibular deficit patients. Moreover, during active gaze shifts, anticipatory mechanisms come into play. Our aim was to explore the extent to which previously described compensatory mechanisms are employed in patients with bilateral vestibular loss.
We used a Video Head Impulse Test (vHIT) to simultaneously record eye and head movements during a video Active Gaze Shift Test (vAGST). Thirty-eight patients with bilateral vestibular deficits and 61 control subjects were tested.
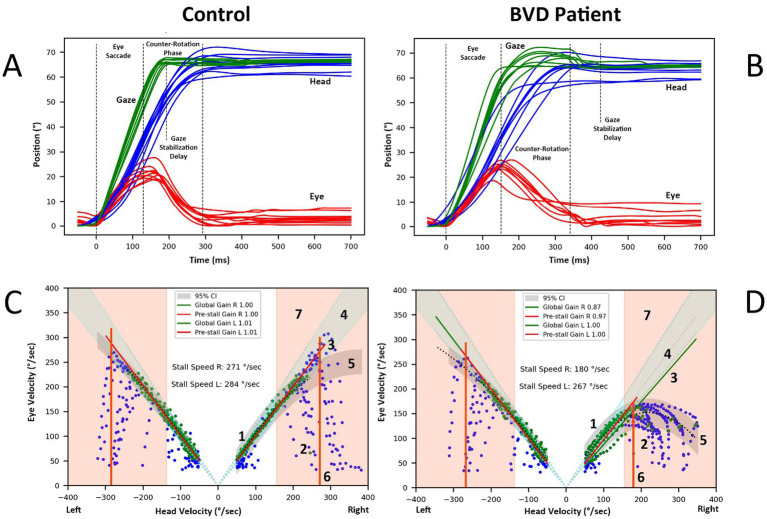
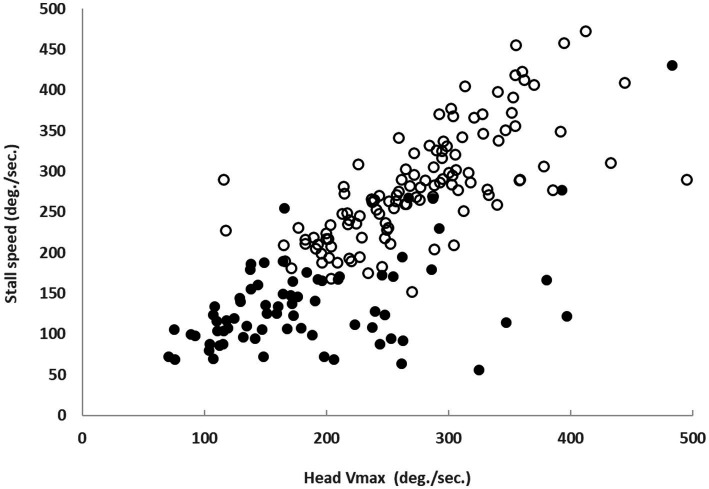
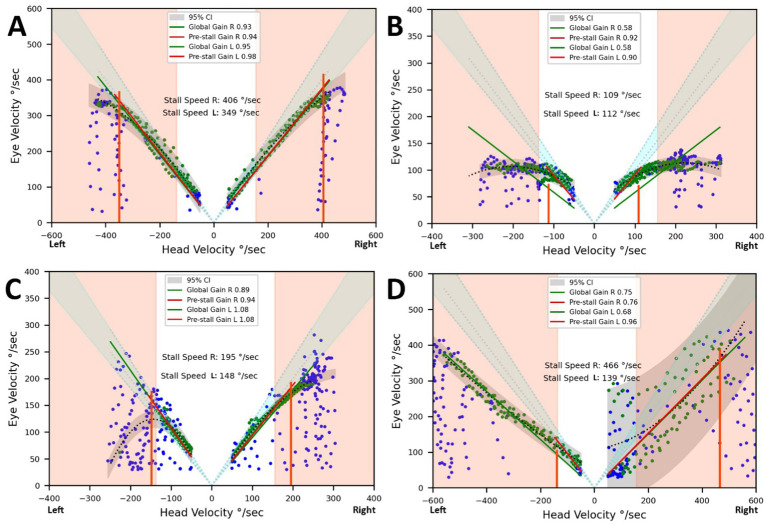
Despite impaired performance on caloric tests and vHIT, most patients exhibited normal gaze stabilization (gain = 0.92 ± 0.1) during active gaze shifts up to a head speed ('stall speed') of approximately 140 ± 60°/sec, compared to 280 ± 65°/sec in controls. Our results indicate that BVD patients spontaneously adopt a head speed during active horizontal movements that significantly improves gaze stabilization compared to passive movements. The stall speed correlates with the spontaneous head speed typically adopted by BVD patients and controls in daily activities. As a consequence of the reduction in head speed and corrective saccades, patients also showed an increased delay in gaze stabilization (413 ± 105 ms in BVD patients versus 358 ± 82 ms in controls) at the end of the gaze shift, which might become disabling for certain tasks.
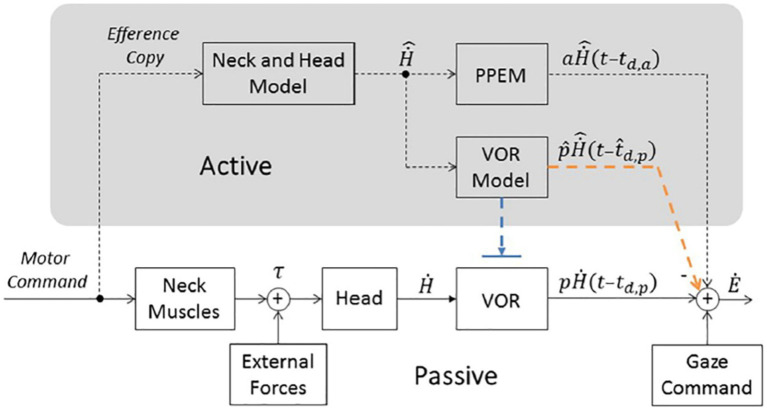
Recent model suggests that compensatory eye movements, which stabilize gaze during the counter rotation phase of active gaze shifts, are predictive in nature. vAGST is not designed to provide an etiological diagnosis but rather a functional assessment of the patient's ability to generate predictive eye movements that compensate for vestibular sensor deficits. Understanding the quality of the patient's sensory predictions can also shed light on vestibular symptoms, even in cases where no vestibular sensor deficit is detected. This suggest that quality of life and oscillopsia questionnaires should distinguish between predictable and unpredictable movements.
虽然日常生活中的大多数头部运动是主动的,但大多数用于评估前庭功能障碍的工具依赖于被动头部运动。单一的增益值不足以量化前庭功能障碍患者主动运动期间的注视稳定效率。此外,在主动注视转移期间,预期机制会发挥作用。我们的目的是探讨双侧前庭丧失患者在多大程度上采用了先前描述的代偿机制。
我们使用视频头脉冲试验(vHIT)在视频主动注视转移试验(vAGST)期间同时记录眼睛和头部运动。对38例双侧前庭功能障碍患者和61名对照受试者进行了测试。
尽管在冷热试验和vHIT中表现受损,但大多数患者在主动注视转移期间,直至头部速度(“失速速度”)约为140±60°/秒时,表现出正常的注视稳定(增益 = 0.92±0.1),而对照组为280±65°/秒。我们的结果表明,与被动运动相比,双侧前庭功能障碍(BVD)患者在主动水平运动期间自发采用的头部速度显著提高了注视稳定。失速速度与BVD患者和对照组在日常活动中通常采用的自发头部速度相关。由于头部速度降低和矫正性扫视,患者在注视转移结束时还表现出注视稳定延迟增加(BVD患者为413±105毫秒,对照组为358±82毫秒),这对于某些任务可能会造成障碍。
最近的模型表明,在主动注视转移的反向旋转阶段稳定注视的代偿性眼球运动本质上是预测性的。vAGST并非旨在提供病因诊断,而是对患者产生预测性眼球运动以补偿前庭传感器缺陷的能力进行功能评估。了解患者感觉预测的质量也可以阐明前庭症状,即使在未检测到前庭传感器缺陷的情况下也是如此。这表明生活质量和视振荡问卷应区分可预测和不可预测的运动。