Warsop Zakary, Anand Nikhil, Al Maliki Husam, De Souza Shuell, Kamyab Arya, Al Hadad Amin, Alrubaiy Laith
Gastroenterology and Hepatology Department, Imperial College London, London SW7 2AZ, UK.
Healthpoint Hospital, Abu Dhabi 112308, United Arab Emirates.
J Pers Med. 2024 Nov 30;14(12):1133. doi: 10.3390/jpm14121133.
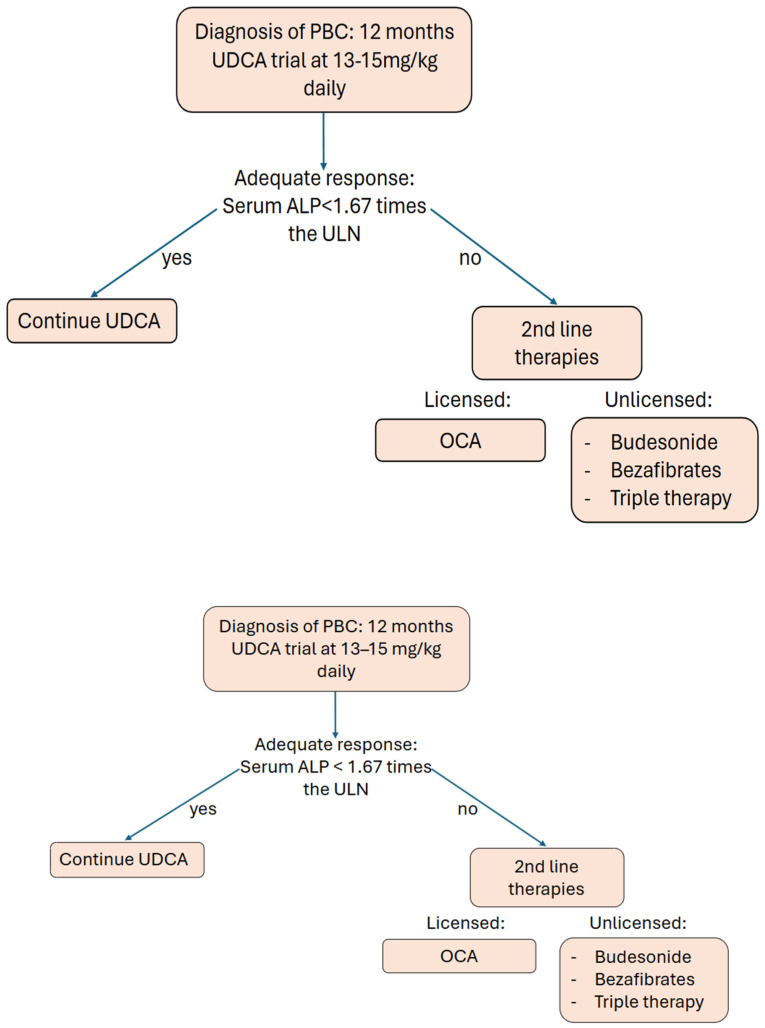
Primary biliary cholangitis (PBC) is an autoimmune chronic cholestatic disease of the liver that symptomatically can present with pruritus and fatigue. Its established first- and second-line therapies are ursodeoxycholic acid (UDCA) and obeticholic acid (OCA) although they provide limited symptom management. Liver transplantation offers a potentially curative therapeutic option in refractory cases progressing to cirrhosis. Novel research published after the current guidelines highlights the importance of providing an up-to-date analysis of treatment options available. In this study, we conducted a literature search using Pubmed, Ovid Medline, and SCOPUS to provide a narrative review of first-line, second-line, and emerging therapies in PBC. UDCA has been well established as a long-term, safe therapy within the literature although it is possible that treatment dosage can be further optimised in refractory patients. It has a favourable side effect profile. Despite improving biochemical markers, histopathological profile, and overall outcomes, up to 30-40% of patients are refractory to it. Age and sex are highlighted as independent indicators of non-responsiveness. This necessitates effective second-line therapies. Future trials could aim to investigate UDCA as a co-first-line therapy. Further supporting results for OCA were found in the interim extension trial of the seminal POISE study. The long-term phase 4 COBOLT trial is still awaiting results to further assess the complications, adherence, and potential adverse effects. It is a viable option in UDCA-refractory patients. The high incidence rate of dose-related pruritis indicates that alternative second-line options are needed. Bezafibrate is an off-label antilipemic agent that shows promise as a prospective second-line therapy option. The landmark BEZURSO trial alleviated some efficacy and safety concerns, but it remains associated with elevated serum creatinine; thus, it should be considered with caution. Other prospective second-line therapies are budesonide, triple therapy, and novel agents such as seladelpar and elafibranor. UDCA should remain the treatment of choice for PBC, though perhaps not as monotherapy. With further investigation, BF shows promise as a new second-line therapy alongside OCA, which it may outperform.
原发性胆汁性胆管炎(PBC)是一种肝脏自身免疫性慢性胆汁淤积性疾病,症状表现为瘙痒和疲劳。其已确立的一线和二线治疗药物是熊去氧胆酸(UDCA)和奥贝胆酸(OCA),尽管它们对症状的控制有限。肝移植为难治性病例进展至肝硬化提供了一种潜在的治愈性治疗选择。当前指南发布后发表的新研究强调了对现有治疗选择进行最新分析的重要性。在本研究中,我们使用PubMed、Ovid Medline和SCOPUS进行文献检索,以对PBC的一线、二线和新兴治疗方法进行叙述性综述。UDCA在文献中已被确立为一种长期、安全的治疗方法,尽管难治性患者的治疗剂量可能需要进一步优化。它具有良好的副作用谱。尽管UDCA能改善生化指标、组织病理学特征和总体预后,但仍有30%-40%的患者对其难治。年龄和性别被认为是无反应的独立指标。这就需要有效的二线治疗方法。未来的试验可以旨在研究将UDCA作为联合一线治疗方法。在开创性的POISE研究的中期扩展试验中发现了更多支持OCA的结果。长期的4期COBOLT试验仍在等待结果,以进一步评估并发症、依从性和潜在的不良反应。对于UDCA难治的患者,它是一种可行的选择。与剂量相关的瘙痒发生率较高,这表明需要其他二线选择。苯扎贝特是一种未获批准的降血脂药物,显示出有望成为一种前瞻性的二线治疗选择。具有里程碑意义的BEZURSO试验缓解了一些疗效和安全性方面的担忧,但它仍与血清肌酐升高有关;因此,应谨慎考虑使用。其他前瞻性的二线治疗方法包括布地奈德、三联疗法以及塞拉地帕和依拉非诺等新型药物。UDCA仍应是PBC的首选治疗药物,不过可能不应作为单一疗法。随着进一步研究,苯扎贝特与OCA一样有望成为一种新的二线治疗方法,甚至可能表现更优。