Tsukamoto Tadashi, Kunimoto Tomohiro, Kaizaki Ryoji
Department of Surgery, Osaka City Juso Hospital, Osaka, Japan.
Department of Surgery, Osaka City Juso Hospital, Osaka, Japan.
Int J Surg Case Rep. 2025 Jan;126:110772. doi: 10.1016/j.ijscr.2024.110772. Epub 2024 Dec 24.
Type 1 gallbladder perforation (GBP) in the free abdominal cavity causes pan-peritonitis, which is both rare and difficult to diagnose.
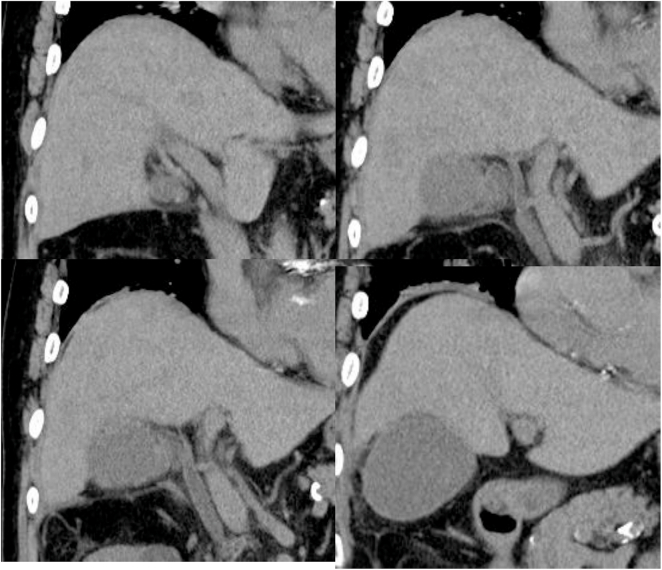
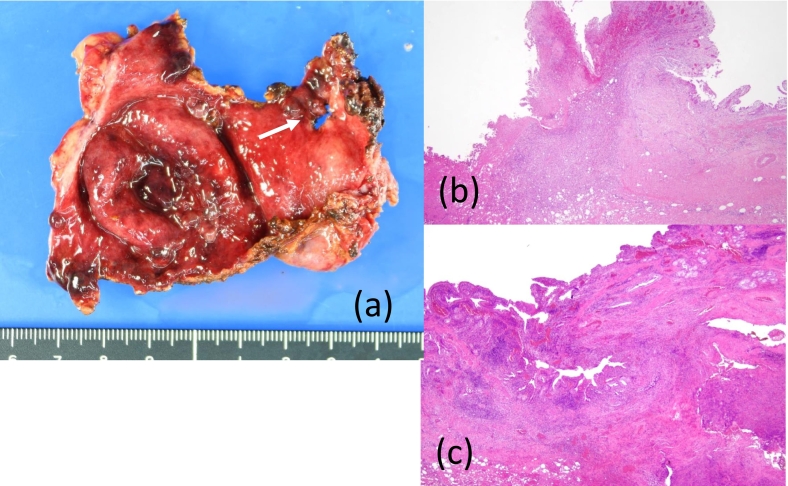
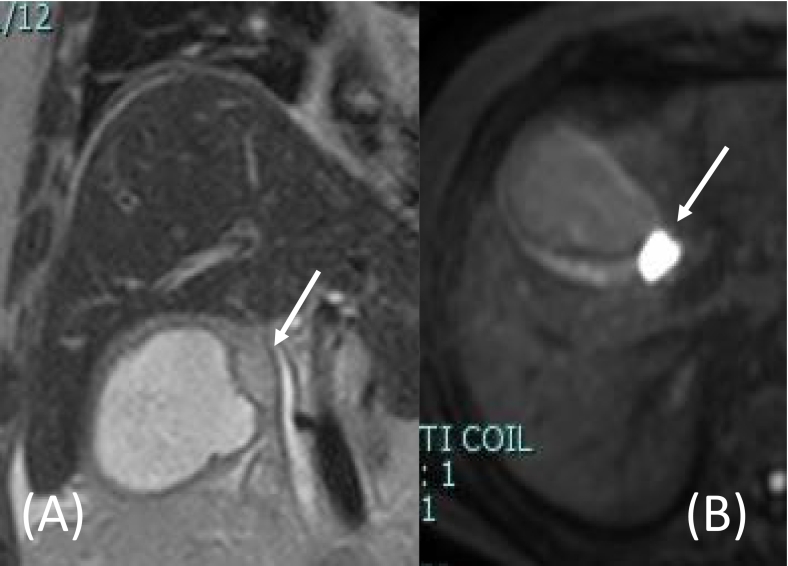
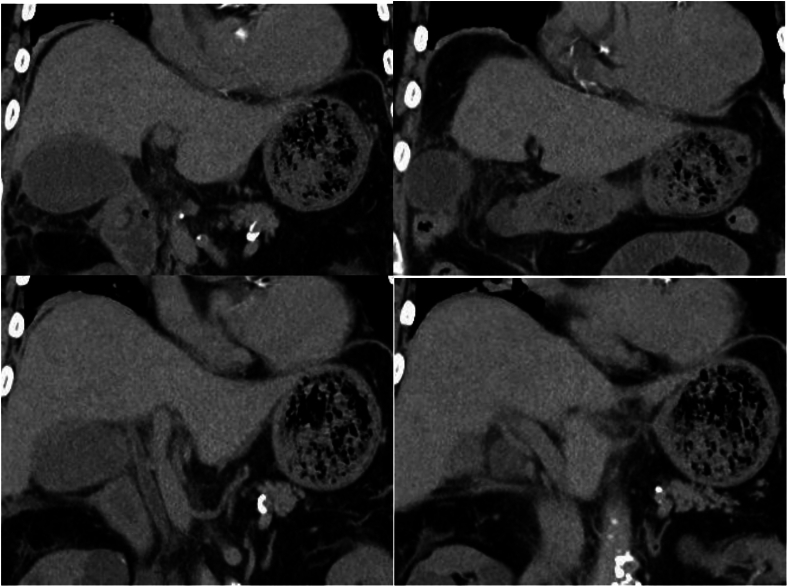
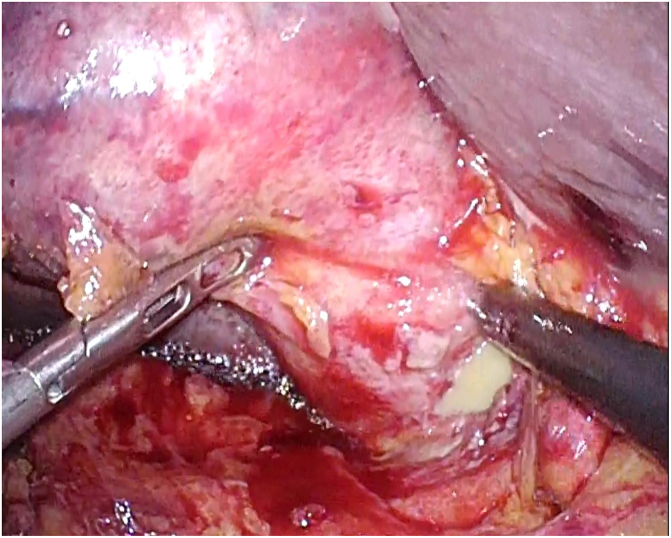
An 80-year-old man presented to our hospital with acute left upper abdominal pain. Twenty days prior to presentation, he had been admitted for 12 days with coronavirus disease 2019 (COVID-19). The patient had mild cholecystitis and received conservative therapy for COVID-19. Upon readmission, his abdomen was flat and soft except for local peritonitis in the left upper abdomen. An emergency laparoscopy revealed a perforation in the ventral wall of the gallbladder neck discharging pus under the lateral lobe of the liver without a gastrointestinal perforation. Therefore, a laparoscopic cholecystectomy and intra-abdominal lavage were performed. Based on the clinical and pathological findings, the GBP was suspected to be a rupture of the abscess in the Rokitansky-Aschoff sinus observed on magnetic resonance imaging during the first admission.
In this case, acute cholecystitis was suppressed by conservative therapy, leaving adhesions of the surrounding tissue and viscus to the gallbladder fundus and body as well as an abscess in the wall of the neck. This was the cause of the GBP and resulted in local peritonitis within the left upper abdomen.
Type 1 GBP develops suddenly and cannot be predicted. In cases of acute cholecystitis once suppressed by conservative therapy and accompanied by cystic formation in the gallbladder wall, early cholecystectomy is recommended considering the risk of GBP.
腹腔游离性1型胆囊穿孔(GBP)可导致全腹膜炎,这种情况既罕见又难以诊断。
一名80岁男性因急性左上腹疼痛入住我院。就诊前20天,他因2019冠状病毒病(COVID-19)入院12天。患者患有轻度胆囊炎,并接受了COVID-19的保守治疗。再次入院时,除左上腹局部腹膜炎外,他的腹部平坦且柔软。急诊腹腔镜检查发现胆囊颈部前壁穿孔,有脓液在肝外侧叶下方流出,无胃肠道穿孔。因此,进行了腹腔镜胆囊切除术和腹腔灌洗。根据临床和病理结果,怀疑该GBP是首次入院时磁共振成像上观察到的罗-阿窦脓肿破裂。
在本病例中,急性胆囊炎经保守治疗得到控制,导致周围组织和脏器与胆囊底部和体部粘连,以及胆囊颈部壁出现脓肿。这是GBP的原因,并导致左上腹局部腹膜炎。
1型GBP发病突然且无法预测。对于曾经保守治疗控制的急性胆囊炎病例,若胆囊壁伴有囊性形成,考虑到GBP的风险,建议早期行胆囊切除术。