Fathallah Ibrahim, Qatza Ayham, Alajrd Abd Alrhman, Al-Ali Majd
Faculty of Medicine, Al-Baath University, Homs, Syria.
Faculty of Medicine, Hama University, Hama, Syria.
Int J Surg Case Rep. 2025 Jan;126:110804. doi: 10.1016/j.ijscr.2024.110804. Epub 2024 Dec 29.
Placenta previa (PP) is characterized by abnormal placental placement in the lower uterine segment, obstructing the cervical opening. Placenta previa totalis (PPT) occurs when the placenta completely covers the internal cervical os. This condition can lead to placenta accreta spectrum (PAS), where the placenta adheres abnormally to the uterine wall, complicating separation. PAS is reported in approximately 0.2 % of pregnancies.
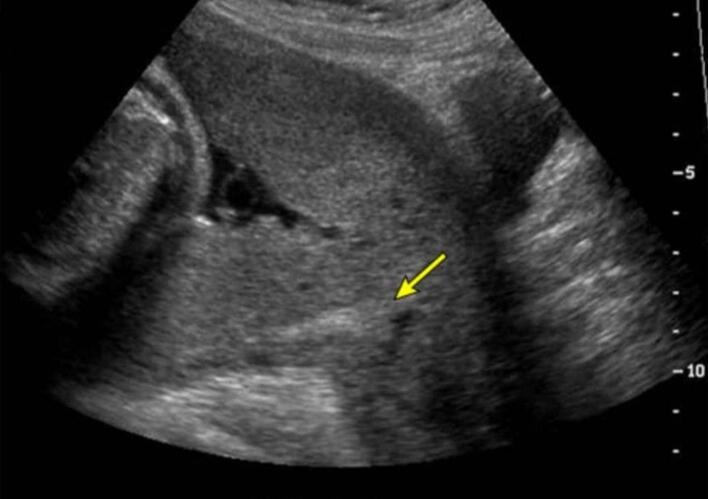
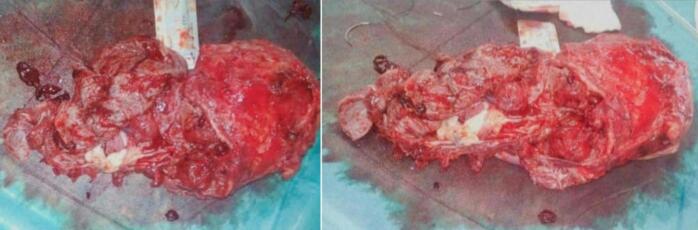
This report concerns a case of a 28-year-old woman at 35 weeks gestation presented with painless vaginal bleeding and contractions. She had a history of five cesarean sections. Ultrasound revealed PPT with suspected placenta percreta, alongside multiple false knots and blood lakes in the placenta. A vertical uterine incision allowed for the delivery of a 2700-g male fetus, with APGAR scores of 9/10 and 10/10. Following massive hemorrhage, an abdominal hysterectomy was performed. The patient was discharged on postoperative day four in stable condition, and the infant was also discharged healthy.
PAS poses significant maternal risks, necessitating early diagnosis and meticulous surgical planning. Management strategies, including feeder vessel ligation and conservative approaches, aim to minimize hemorrhage. Hysterectomy remains a critical intervention in cases of uncontrollable bleeding, with postoperative care focused on hemodynamic stabilization and pain management.
This paper emphasizes effective communication, timely decision-making, and adherence to massive hemorrhage protocols in managing obstetric emergencies like PAS. In addition, routine screening during second-trimester ultrasounds for high-risk pregnancies and further prospective clinical trials are needed to enhance diagnostic and management strategies.
前置胎盘(PP)的特征是胎盘在子宫下段异常着床,阻塞宫颈口。完全性前置胎盘(PPT)是指胎盘完全覆盖宫颈内口。这种情况可导致胎盘植入谱系疾病(PAS),即胎盘异常附着于子宫壁,导致胎盘剥离困难。据报道,PAS在妊娠中的发生率约为0.2%。
本报告涉及一名28岁、孕35周的女性,出现无痛性阴道出血和宫缩。她有五次剖宫产史。超声检查显示为完全性前置胎盘,疑似穿透性胎盘植入,同时胎盘内有多个假结和血湖。经腹纵切口娩出一名体重2700克的男婴,阿氏评分分别为9/10和10/10。在大量出血后,行腹式子宫切除术。患者术后第4天病情稳定出院,婴儿也健康出院。
PAS对母亲有重大风险,需要早期诊断和精心的手术规划。管理策略包括结扎供血血管和采取保守方法,旨在尽量减少出血。子宫切除术仍然是控制出血病例中的关键干预措施,术后护理重点是血流动力学稳定和疼痛管理。
本文强调在处理像PAS这样的产科紧急情况时,要进行有效的沟通、及时的决策并遵守大出血处理方案。此外,需要在孕中期超声检查时对高危妊娠进行常规筛查,并开展进一步的前瞻性临床试验,以加强诊断和管理策略。