Zhang Yidan, Xu Yingqi, Xu Jianlin, Zhong Hua, Xia Jinjing, Zhong Runbo
Department of Respiratory and Critical Care Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Cancer Sci. 2025 Mar;116(3):753-763. doi: 10.1111/cas.16437. Epub 2024 Dec 31.
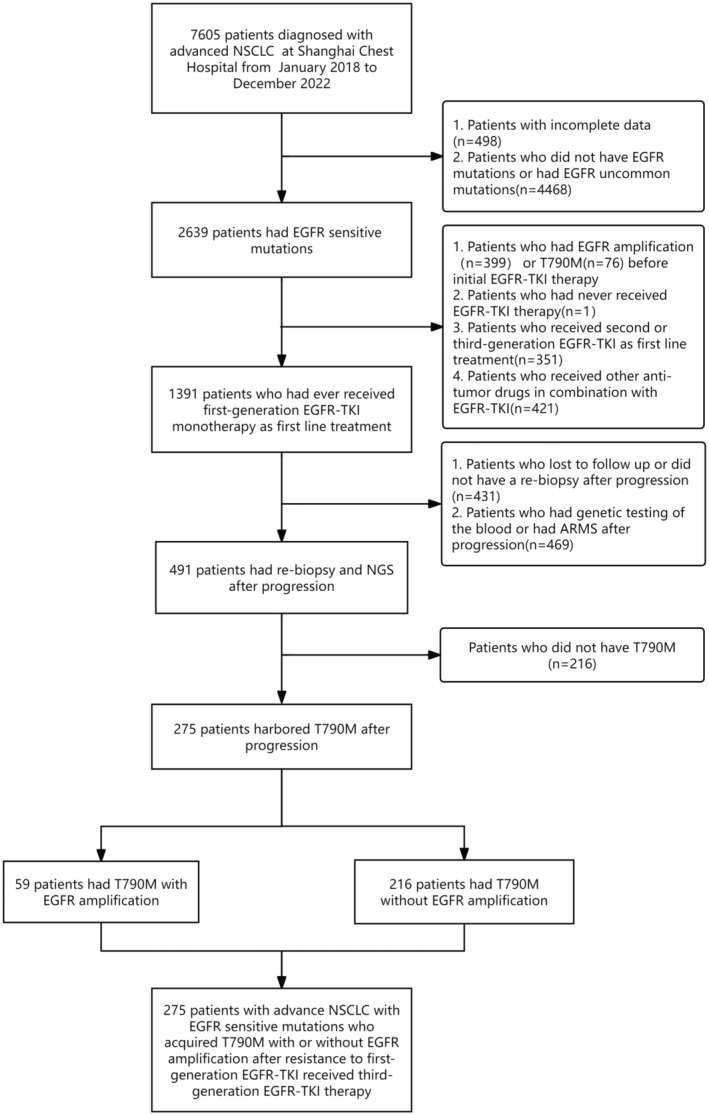
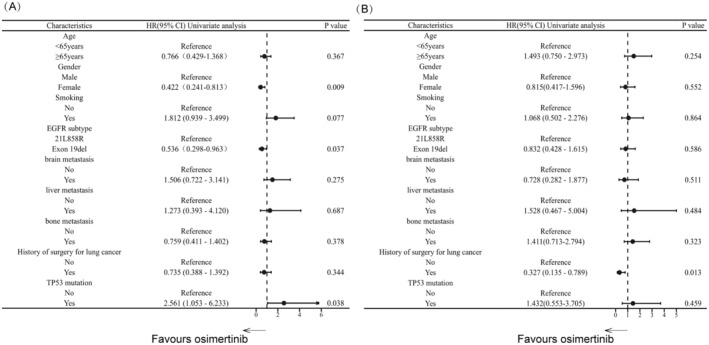
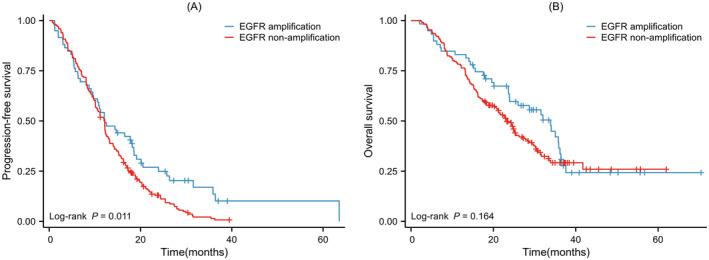
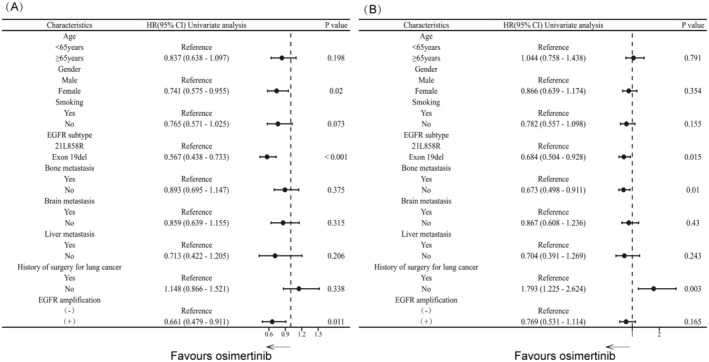
Third-generation epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) is the standard therapy for patients harboring T790M after first-generation EGFR-TKI resistance. However, the impact of acquired EGFR amplification on the efficacy of third-generation EGFR-TKI against T790M remains uncertain. We aimed to investigate whether the presence of acquired EGFR amplification after first-generation EGFR-TKI resistance influences the efficacy of third-generation EGFR-TKI in patients with advanced non-small-cell lung cancer (NSCLC). We reviewed data from 275 advanced NSCLC patients harboring T790M after first-generation EGFR-TKI resistance. Patients were categorized into two groups based on the presence or absence of acquired EGFR amplification identified through next-generation sequencing (NGS) after first-line EGFR-TKI treatment. We evaluated the efficacy of osimertinib used as a second-line treatment. Among these patients, 59 exhibited acquired EGFR amplification, while 216 did not. The median progression-free survival (PFS) was 12.20 months in the EGFR amplification group and 12.03 months in the non-amplification group (p = 0.011), with median overall survival (OS) of 33.90 months and 23.30 months, respectively (p = 0.164). Multivariate analysis of PFS revealed that acquired EGFR amplification and EGFR 19del were independent prognostic factors for patients with T790M undergoing osimertinib. Additionally, subgroup analysis indicated a prolonged PFS in patients with EGFR 19del compared to those with EGFR 21L858R (p = 0.034) in the EGFR amplification group. Following first-generation EGFR-TKI resistance, advanced EGFR-mutant NSCLC patients harboring both acquired T790M and EGFR amplification are likely to experience enhanced PFS with osimertinib. This phenomenon is particularly noteworthy among individuals with EGFR 19del.
第三代表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKI)是第一代EGFR-TKI耐药后携带T790M患者的标准治疗方法。然而,获得性EGFR扩增对第三代EGFR-TKI治疗T790M疗效的影响仍不确定。我们旨在研究第一代EGFR-TKI耐药后获得性EGFR扩增的存在是否会影响第三代EGFR-TKI对晚期非小细胞肺癌(NSCLC)患者的疗效。我们回顾了275例第一代EGFR-TKI耐药后携带T790M的晚期NSCLC患者的数据。根据一线EGFR-TKI治疗后通过二代测序(NGS)确定的获得性EGFR扩增的有无,将患者分为两组。我们评估了奥希替尼作为二线治疗的疗效。在这些患者中,59例出现获得性EGFR扩增,216例未出现。EGFR扩增组的中位无进展生存期(PFS)为12.20个月,非扩增组为12.03个月(p = 0.011),中位总生存期(OS)分别为33.90个月和23.30个月(p = 0.164)。PFS的多因素分析显示,获得性EGFR扩增和EGFR 19del是接受奥希替尼治疗的T790M患者的独立预后因素。此外,亚组分析表明,在EGFR扩增组中,与EGFR 21L858R患者相比,EGFR 19del患者的PFS延长(p = 0.034)。第一代EGFR-TKI耐药后,同时携带获得性T790M和EGFR扩增的晚期EGFR突变NSCLC患者使用奥希替尼可能会有更长的PFS。这种现象在EGFR 19del患者中尤为值得注意。