Miguel Maria João, Robalo Nunes Tomás, Gomes André, Boavida Susana, Marques Nuno
Infectious Diseases, Hospital Garcia de Orta, Lisbon, PRT.
Cureus. 2024 Dec 3;16(12):e75039. doi: 10.7759/cureus.75039. eCollection 2024 Dec.
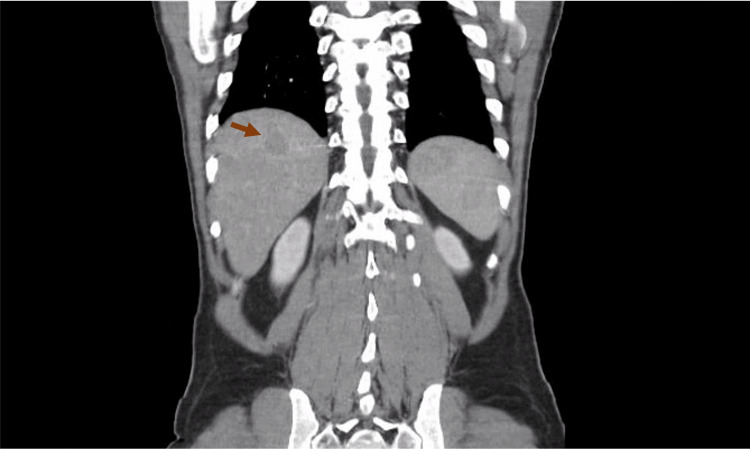
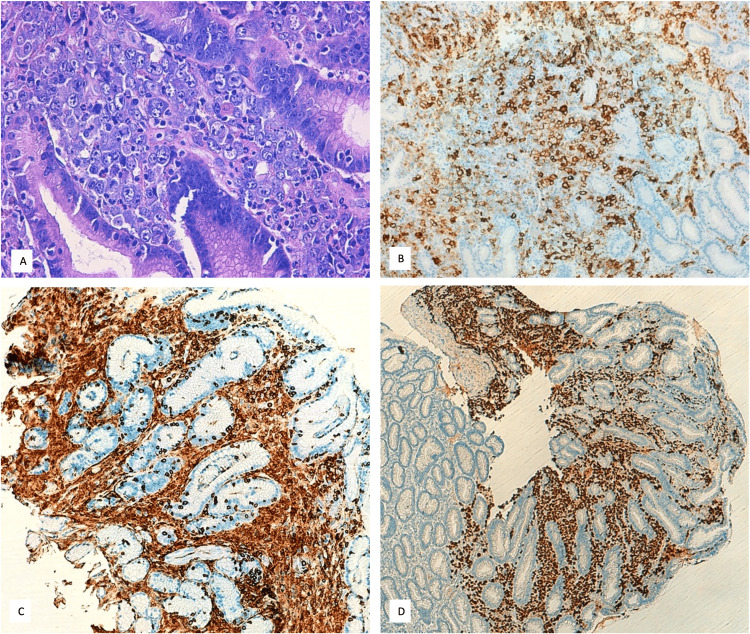
Extra-cavitary primary effusion lymphoma (PEL), often associated with human herpes virus 8 (HHV8) infection, represents a rare and aggressive form of non-Hodgkin lymphoma, which is predominantly found in individuals with severe immunosuppression. As an acquired immunodeficiency syndrome (AIDS)-associated lymphoma, PEL typically manifests in the context of advanced human immunodeficiency virus (HIV) infection, requiring tailored therapeutic approaches to manage both the lymphoma and underlying immunodeficiency. A 53-year-old male patient from Cape Verde presented with a three-day history of fever, night sweats, right iliac fossa pain, hematochezia, and an unintentional weight loss of five kilograms over the previous two months. A laboratory study revealed a previously undiagnosed co-infection with HIV-1 and HIV-2, with a CD4+ T-cell count of 63/μL. The abdominal-pelvic computed tomography (CT) scan revealed hepatosplenomegaly with hypodense nodular lesions and prominent lymph nodes in the celiac-mesenteric, axillary, and cervical regions. Lung imaging showed non-specific nodules. An extensive investigation for opportunistic infections was conducted, with a bronchoalveolar lavage culture test positive for and a colon biopsy indicating Cytomegalovirus colitis. Further histological examination from a gastric biopsy revealed the diagnosis of the solid variant of PEL. The patient initiated treatment for opportunistic infections followed by antiretroviral therapy. However, he experienced multiple complications and due to his deteriorating condition, chemotherapy was not initiated and he ultimately died. This rare clinical case of lymphoma in a patient co-infected with HIV-1 and HIV-2, the first of its kind to be reported, to the authors' knowledge, underscores the diagnostic and therapeutic challenges associated with this condition.
腔外原发性渗出性淋巴瘤(PEL)通常与人类疱疹病毒8型(HHV8)感染相关,是一种罕见且侵袭性的非霍奇金淋巴瘤,主要见于严重免疫抑制的个体。作为一种与获得性免疫缺陷综合征(AIDS)相关的淋巴瘤,PEL通常在晚期人类免疫缺陷病毒(HIV)感染的背景下出现,需要采用针对性的治疗方法来处理淋巴瘤和潜在的免疫缺陷。一名来自佛得角的53岁男性患者,有三天发热、盗汗、右下腹疼痛、便血病史,且在过去两个月内无意体重减轻了5公斤。实验室检查发现先前未诊断出的HIV-1和HIV-2合并感染,CD4 + T细胞计数为63/μL。腹盆腔计算机断层扫描(CT)显示肝脾肿大,伴有低密度结节性病变,腹腔肠系膜、腋窝和颈部区域有明显淋巴结肿大。肺部影像学显示非特异性结节。对机会性感染进行了广泛调查,支气管肺泡灌洗培养试验呈阳性,结肠活检提示巨细胞病毒性结肠炎。胃活检的进一步组织学检查确诊为PEL实体变体。患者开始接受机会性感染治疗,随后接受抗逆转录病毒治疗。然而,他出现了多种并发症,由于病情恶化,未开始化疗,最终死亡。据作者所知,这例HIV-1和HIV-2合并感染患者的罕见淋巴瘤临床病例是首例报告,凸显了与这种情况相关的诊断和治疗挑战。