Attias Mikhaël, Alvarez Fernando, Al-Aubodah Tho-Alfakar, Istomine Roman, McCallum Paige, Huang Fan, Sleiman Abrahim, Nishimura Tamiko, Del Rincón Sonia V, Riazalhosseini Yasser, Piccirillo Ciriaco A
Department of Microbiology and Immunology, McGill University, Montreal, Quebec, Canada.
Infectious Diseases and Immunity in Global Health (IDIGH) Program, Centre for Translation Biology (CTB), The Research Institute of the McGill University Health Centre (RI-MUHC), Montreal, Quebec, Canada.
J Immunother Cancer. 2025 Jan 6;13(1):e009435. doi: 10.1136/jitc-2024-009435.
Immune checkpoint inhibitors targeting programmed cell death protein-1 (PD-1) are the first line of treatment for many solid tumors including melanoma. PD-1 blockade enhances the effector functions of melanoma-infiltrating CD8 T cells, leading to durable tumor remissions. However, 55% of patients with melanoma do not respond to treatment. As Foxp3 regulatory T (T) cells play an important role in tumor-induced immunosuppression and express PD-1, we hypothesized that anti-PD-1 also increases the functions of melanoma-infiltrating T cells, which could be detrimental to treatment efficacy.
The cellular and functional dynamics of T cells were evaluated in C57Bl/6 Foxp3-reporter mice bearing highly immunogenic and PD-1 blockade-sensitive Yale University Mouse Melanoma Exposed to Radiation 1.7 (YUMMER1.7) tumors. T cell responses in tumors and lymphoid compartments were examined throughout tumor growth or therapy and were assessed ex vivo by multiparametric flow cytometry analysis, with in vitro suppression assays using tumor-infiltrating lymphocytes isolated by fluorescence-activated cell sorting (FACS) and through spatial proteomic and transcriptomic profiling.
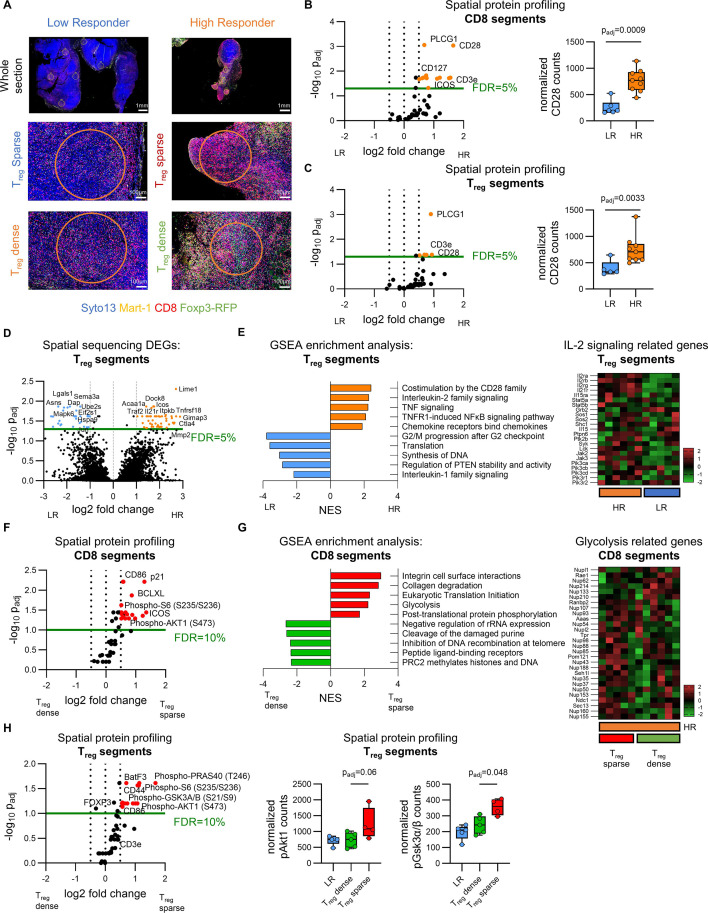
In this highly immunogenic melanoma model, anti-PD-1 monotherapy yielded high responders (HRs) and low responders (LRs). We show that the potent CD8 T cell responses characteristic of HR tumors paradoxically coincide with the expansion of highly-activated, Helios-expressing T cells. In both HRs and LRs, T cells co-localize with CD8 T cells in immunogenic regions of the tumor and display potent suppressive capacity in vitro. Further characterization revealed that melanoma-infiltrating T cells progressively acquire T-bet and interferon gamma expression, exclusively in HRs, and induction of this T helper cell 1 (T1)-like phenotype in vitro led to CD8 T cell evasion from T cell-mediated suppression. Using spatial proteomic and transcriptomic profiling, we demonstrate that T cells display an increased activity of PI3K/Akt signaling in regions of HR tumors with an elevated CD8:T cell ratio.
PD-1 blockade promotes the expansion of a subset of highly-activated T cells coexpressing PD-1 and Helios. While these cells are potently suppressive outside tumor environments, costimulatory and inflammatory signals present in the tumor microenvironment lead to their local acquisition of T1-like characteristics and loss of suppression of effector T cells.
靶向程序性细胞死亡蛋白1(PD-1)的免疫检查点抑制剂是包括黑色素瘤在内的许多实体瘤的一线治疗方法。PD-1阻断增强了浸润黑色素瘤的CD8 T细胞的效应功能,从而导致持久的肿瘤缓解。然而,55%的黑色素瘤患者对治疗无反应。由于Foxp3调节性T(T)细胞在肿瘤诱导的免疫抑制中起重要作用并表达PD-1,我们推测抗PD-1也会增加浸润黑色素瘤的T细胞功能,这可能对治疗效果不利。
在携带高免疫原性且对PD-1阻断敏感的耶鲁大学暴露于辐射的小鼠黑色素瘤1.7(YUMMER1.7)肿瘤的C57Bl/6 Foxp3报告基因小鼠中评估T细胞的细胞和功能动态。在肿瘤生长或治疗过程中检查肿瘤和淋巴区室中的T细胞反应,并通过多参数流式细胞术分析进行体外评估,使用通过荧光激活细胞分选(FACS)分离的肿瘤浸润淋巴细胞进行体外抑制试验,并通过空间蛋白质组学和转录组学分析。
在这个高免疫原性黑色素瘤模型中,抗PD-1单药治疗产生了高反应者(HRs)和低反应者(LRs)。我们表明,HR肿瘤特有的强大CD8 T细胞反应与高激活、表达Helios的T细胞的扩增自相矛盾地同时出现。在HRs和LRs中,T细胞在肿瘤的免疫原性区域与CD8 T细胞共定位,并在体外显示出强大的抑制能力。进一步表征显示,浸润黑色素瘤的T细胞仅在HRs中逐渐获得T-bet和干扰素γ表达,并且在体外诱导这种辅助性T细胞1(T1)样表型导致CD8 T细胞逃避T细胞介导的抑制。使用空间蛋白质组学和转录组学分析,我们证明T细胞在CD8:T细胞比率升高的HR肿瘤区域显示出PI3K/Akt信号传导活性增加。
PD-1阻断促进了共表达PD-1和Helios的高激活T细胞亚群的扩增。虽然这些细胞在肿瘤外环境中具有强大的抑制作用,但肿瘤微环境中存在的共刺激和炎症信号导致它们在局部获得T1样特征并失去对效应T细胞的抑制作用。