Massimo Gianmichele, Dyson Nicki, Olotu Fisayo, Khambata Rayomand S, Ahluwalia Amrita
Barts & The London Faculty of Medicine & Dentistry, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ, UK.
Antioxidants (Basel). 2024 Nov 22;13(12):1439. doi: 10.3390/antiox13121439.
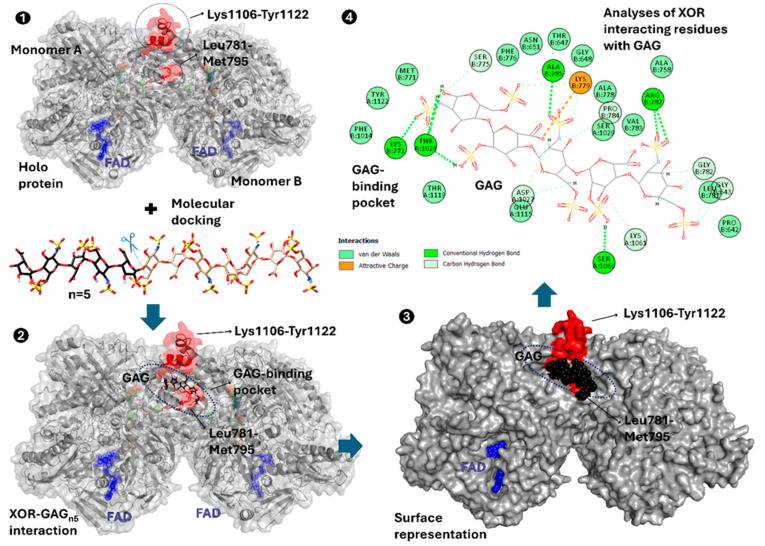
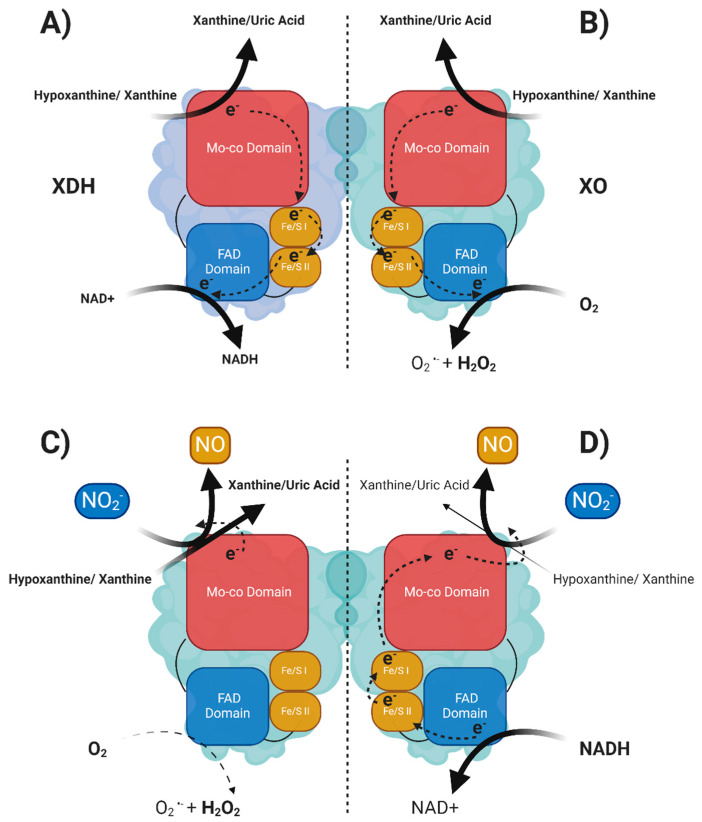
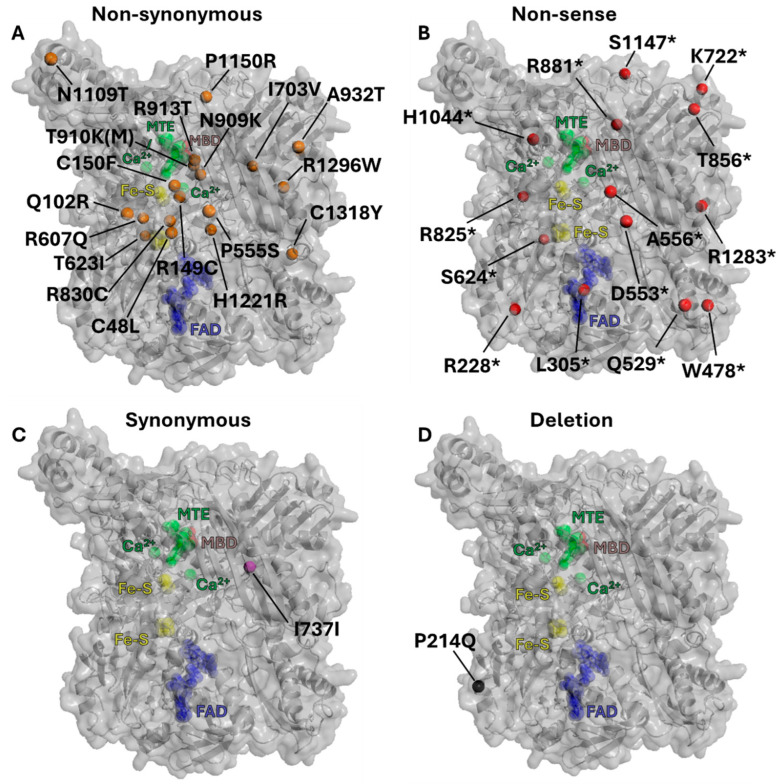
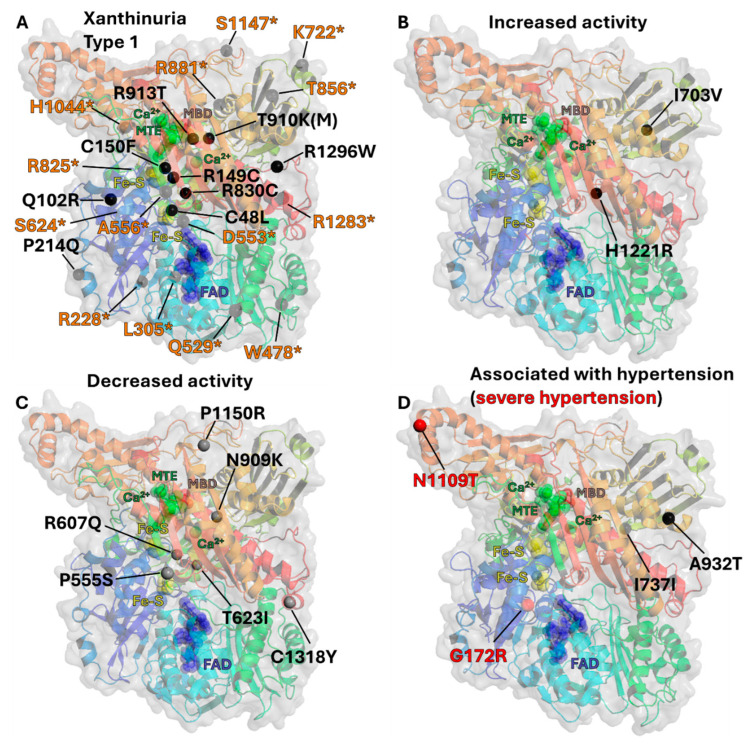
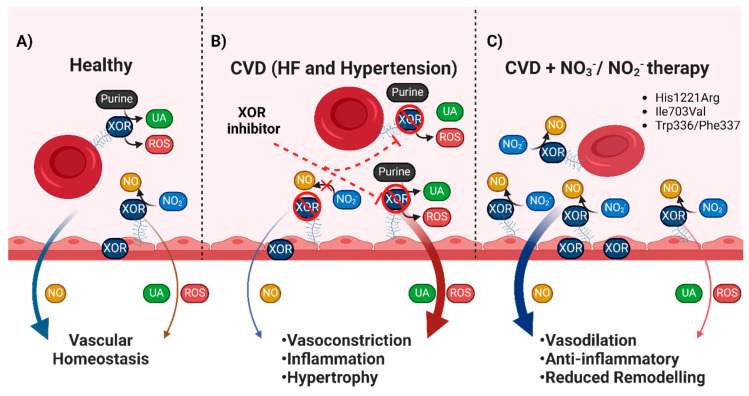
The majority of naturally occurring mutations of the human gene , are associated with reduced or completely absent xanthine oxidoreductase (XOR) activity, leading to a disease known as classical xanthinuria, which is due to the accumulation and excretion of xanthine in urine. Three types of classical xanthinuria have been identified: type I, characterised by XOR deficiency, type II, caused by XOR and aldehyde oxidase (AO) deficiency, and type III due to XOR, AO, and sulphite oxidase (SO) deficiency. Type I and II are considered rare autosomal recessive disorders, a condition where two copies of the mutated gene must be present to develop the disease or trait. In most cases, xanthinuria type I and II result to be asymptomatic, and only occasionally lead to renal failure due to urolithiasis caused by xanthine deposition. However, in the last 10-15 years, new observations have been made about the link between naturally occurring mutations and pathological phenotypes particularly pertinent to cardiovascular diseases (CVD). These links have been attributed to a genetically driven increase of XOR expression and activity that is responsible for what is thought to be damaging uric acid (UA) and reactive oxygen species (ROS) accumulation, nitric oxide (·NO) depletion and endothelial dysfunction. In this review, we discuss the importance of genetics for interindividual variability of XOR expression and activity while focusing mainly on those variants thought to be relevant for CVD. In addition, we discuss the potential exploitation of the genetically driven increase of XOR activity to deliver beneficial bioavailable ·NO. Finally, we examine the effect that non-synonymous mutations have on the tertiary structure of the protein and consequently on its capacity to interact with glycosaminoglycans (GAGs) localised on the outer surface of endothelial cells.
人类基因的大多数自然发生的突变与黄嘌呤氧化还原酶(XOR)活性降低或完全缺失有关,导致一种称为经典黄嘌呤尿症的疾病,这是由于黄嘌呤在尿液中的积累和排泄所致。已鉴定出三种类型的经典黄嘌呤尿症:I型,其特征为XOR缺乏;II型,由XOR和醛氧化酶(AO)缺乏引起;III型,由于XOR、AO和亚硫酸盐氧化酶(SO)缺乏。I型和II型被认为是罕见的常染色体隐性疾病,即必须存在两个拷贝的突变基因才会出现该疾病或性状。在大多数情况下,I型和II型黄嘌呤尿症无症状,仅偶尔因黄嘌呤沉积引起的尿路结石导致肾衰竭。然而,在过去10至15年中,人们对自然发生的突变与心血管疾病(CVD)特别相关的病理表型之间的联系有了新的认识。这些联系归因于基因驱动的XOR表达和活性增加,这被认为是导致尿酸(UA)和活性氧(ROS)积累、一氧化氮(·NO)消耗以及内皮功能障碍的原因。在本综述中,我们讨论了遗传学对于XOR表达和活性个体间变异性的重要性,主要关注那些被认为与CVD相关的变体。此外,我们讨论了利用基因驱动的XOR活性增加来递送有益的生物可利用·NO的可能性。最后,我们研究非同义突变对蛋白质三级结构的影响,以及由此对其与位于内皮细胞外表面的糖胺聚糖(GAGs)相互作用能力的影响。