Asai Nobuhiro, Ohashi Wataru, Shibata Yuichi, Sakanashi Daisuke, Kato Hideo, Hagihara Mao, Suematsu Hiroyuki, Mikamo Hiroshige
Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute 480-1195, Aichi, Japan.
Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute 480-1195, Aichi, Japan.
Antibiotics (Basel). 2024 Dec 11;13(12):1205. doi: 10.3390/antibiotics13121205.
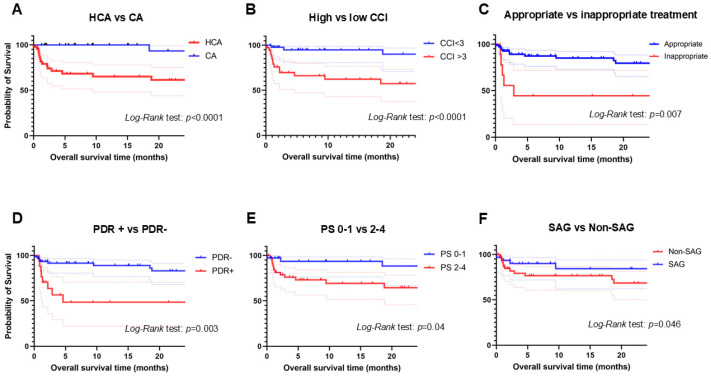
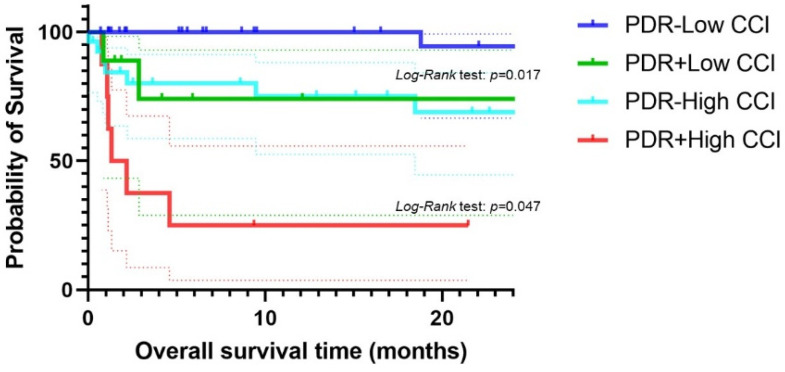
Despite the advancements in diagnostic methods and antibiotic treatment, empyema is a critical respiratory infection, showing a high mortality rate of 10-25%. To evaluate the bacterial etiology and prognostic factors of acute empyema, we conducted this long-term retrospective cohort study at our institute between 2008 and 2022. A total of 80 patients were enrolled in this cohort. The median age was 72 years (range 19 to 93 years), and 61 (76%) were male. The most common underlying disease was malignancy, seen in 28 (35%). The mean Charlson comorbidity index (CCI) was 2.7 (±2.4). The 30-day and in-hospital mortality were 9 (11%) and 15 (19%), respectively. Univariate analysis revealed that healthcare-associated infection, inappropriate treatment, high CCI score, performance status (PS) of 2-4, and isolation of potentially drug-resistant (PDR) pathogens were poor prognostic factors. Finally, multivariate analysis showed that high CCI score ( = 0.009) and isolation of PDR pathogens ( = 0.011) were independent poor prognostic factors for in-hospital death in acute empyema. We found that higher CCI scores and isolation of PDR pathogens were independent poor prognostic factors for in-hospital mortality among empyema patients.
尽管诊断方法和抗生素治疗取得了进展,但脓胸仍是一种严重的呼吸道感染,死亡率高达10%-25%。为了评估急性脓胸的细菌病因和预后因素,我们于2008年至2022年在我院开展了这项长期回顾性队列研究。该队列共纳入80例患者。中位年龄为72岁(范围19至93岁),61例(76%)为男性。最常见的基础疾病是恶性肿瘤,共28例(35%)。Charlson合并症指数(CCI)的平均值为2.7(±2.4)。30天和住院死亡率分别为9例(11%)和15例(19%)。单因素分析显示,医疗相关感染、治疗不当、CCI评分高、2-4级的体能状态(PS)以及分离出潜在耐药(PDR)病原体是不良预后因素。最后,多因素分析表明,CCI评分高( = 0.009)和分离出PDR病原体( = 0.011)是急性脓胸患者住院死亡的独立不良预后因素。我们发现,较高的CCI评分和分离出PDR病原体是脓胸患者住院死亡率的独立不良预后因素。