Lim Su Lin, Tay Melissa, Ang Siew Min, Wai Shu Ning, Ong Kai Wen, Neo Wen Joo, Yap Qai Ven, Chan Yiong Huak, Khoo Chin Meng
Office of Allied Health & Pharmacy, National University Hospital, Singapore 119228, Singapore.
Department of Dietetics, National University Hospital, Singapore 119074, Singapore.
Nutrients. 2024 Dec 19;16(24):4380. doi: 10.3390/nu16244380.
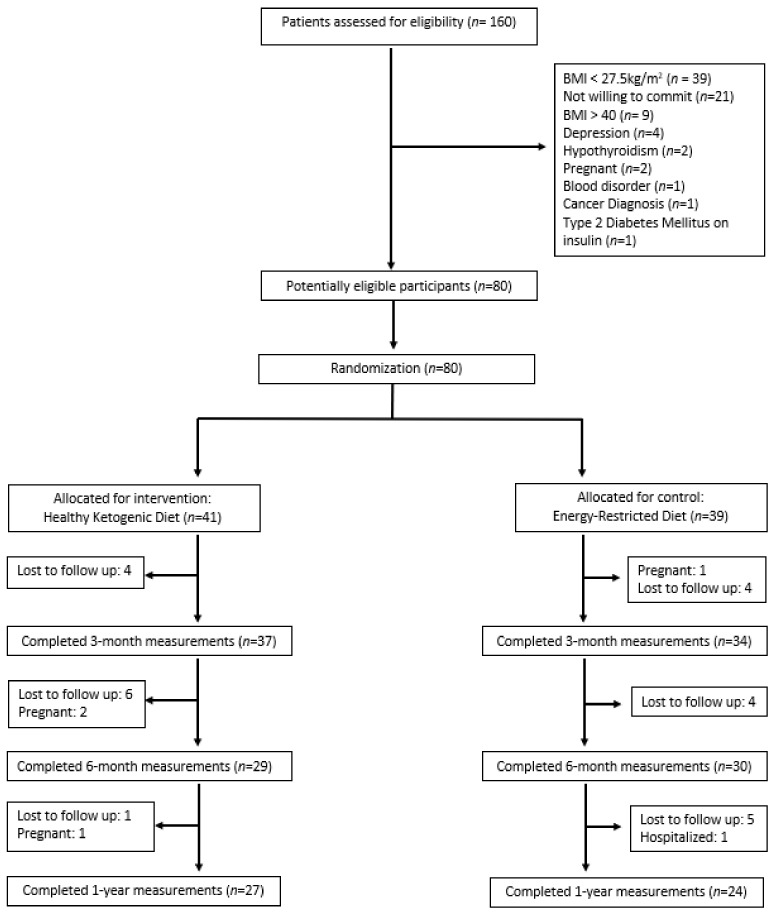
: The ketogenic diet (KD) is widely used for weight management by reducing appetite, enhancing fat oxidation, and facilitating weight loss. However, the high content of total and saturated fats in a conventional KD may elevate low-density lipoprotein (LDL)-cholesterol levels, a known risk factor for cardiovascular diseases, highlighting the need for healthier alternatives. This study aimed to investigate the effect of a newly developed Healthy Ketogenic Diet (HKD) versus an Energy-Restricted Diet (ERD) on weight loss and metabolic outcomes among adults with obesity. : Multi-ethnic Asian adults ( = 80) with body mass index ≥ 27.5 kg/m were randomized either to HKD ( = 41) or ERD = 39) for 6 months. Both groups followed an energy-restricted healthy diet, emphasizing on reducing saturated and trans fats. The HKD group additionally limited net carbohydrate intake to no more than 50 g per day. Dietary adherence was supported via the Nutritionist Buddy app with dietitian coaching. The primary outcome was weight change from baseline at 6 months. Secondary outcomes included weight change at 3 months and 1 year, along with changes in metabolic profiles. Data were analyzed using linear regression with an intention-to-treat approach. : The HKD group achieved significantly greater mean weight loss at 6 months than the ERD group (-7.8 ± 5.2 kg vs. -4.2 ± 5.6 kg, = 0.01). The mean weight loss percentage at 6 months was 9.3 ± 5.9% and 4.9 ± 5.8% for the HKD and ERD groups, respectively ( = 0.004). Improvements in metabolic profiles were also significantly better in the HKD group [glycated hemoglobin (-0.3 ± 0.3% vs. -0.1 ± 0.2%, = 0.008), systolic blood pressure (-7.7 ± 8.9 mmHg vs. -2.6 ± 12.2 mmHg, = 0.005), and aspartate transaminase (-7.6 ± 15.5 IU/L vs. 0.6 ± 11.5 IU/L, = 0.01)], with no increase in LDL-cholesterol (-0.12 ± 0.60 mmol/L vs. -0.04 ± 0.56 mmol/L, = 0.97) observed in either group. : The HKD was more effective than the ERD in promoting weight loss and improving cardiometabolic outcomes without elevation in LDL-cholesterol. It can be recommended for therapeutic intervention in patients with obesity.
生酮饮食(KD)通过降低食欲、增强脂肪氧化和促进体重减轻,被广泛用于体重管理。然而,传统生酮饮食中总脂肪和饱和脂肪含量较高,可能会提高低密度脂蛋白(LDL)胆固醇水平,这是心血管疾病的一个已知风险因素,凸显了对更健康替代方案的需求。本研究旨在调查新开发的健康生酮饮食(HKD)与能量限制饮食(ERD)对肥胖成年人减肥和代谢结果的影响。
多民族亚洲成年人(n = 80),体重指数≥27.5 kg/m²,被随机分为HKD组(n = 41)或ERD组(n = 39),为期6个月。两组均遵循能量限制的健康饮食,强调减少饱和脂肪和反式脂肪。HKD组还将净碳水化合物摄入量限制在每天不超过50克。通过营养师助手应用程序和营养师指导来支持饮食依从性。主要结局是6个月时相对于基线的体重变化。次要结局包括3个月和1年时的体重变化以及代谢指标的变化。采用意向性分析方法,使用线性回归对数据进行分析。
HKD组在6个月时的平均体重减轻显著大于ERD组(-7.8±5.2千克 vs. -4.2±5.6千克,P = 0.01)。HKD组和ERD组在6个月时的平均体重减轻百分比分别为9.3±5.9%和4.9±5.8%(P = 0.004)。HKD组的代谢指标改善也显著更好[糖化血红蛋白(-0.3±0.3% vs. -0.1±0.2%,P = 0.008)、收缩压(-7.7±8.9 mmHg vs. -2.6±12.2 mmHg,P = 0.005)和天冬氨酸转氨酶(-7.6±15.5 IU/L vs. 0.6±11.5 IU/L,P = 0.01)],两组均未观察到LDL胆固醇升高(-0.12±0.60 mmol/L vs. -0.04±0.56 mmol/L,P = 0.97)。
HKD在促进体重减轻和改善心脏代谢结局方面比ERD更有效,且不会升高LDL胆固醇。可推荐用于肥胖患者的治疗干预。