Ahsan Irfan, Hennawi Hussam Al, Bedi Angad, Khan Muhammad Khuzzaim, Duseja Nikhil, Ho Reginald T
Division of Cardiology, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania, USA.
Department of Internal Medicine, Jefferson Abington Hospital, Abington, Pennsylvania, USA.
J Cardiovasc Electrophysiol. 2025 Feb;36(2):501-511. doi: 10.1111/jce.16548. Epub 2025 Jan 7.
Left bundle branch area pacing (LBBAP) is a new technique for patients with atrioventricular block (AVB) and preserved left ventricular ejection fraction (LVEF), potentially offering better cardiac function than right ventricular pacing (RVP).
We searched databases and registries for studies that compared LBBAP with RVP in patients with AVB and preserved LVEF. We extracted data on various outcomes and pooled the effect estimates using random-effects models.
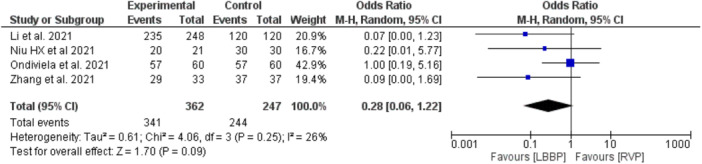
Our meta-analysis included 14 studies (10 observational and 4 RCTs) involving 3062 patients with AVB. The analysis revealed that the QRS duration was significantly shorter in the LBBAP group compared to the RVP group [MD = -35.56 ms; 95% CI: (-39.27, -31.85), p < 0.00001]. Patients in the LBBAP group also exhibited a significant increase in left ventricular ejection fraction (LVEF) [MD = 5.48%; 95% CI: (4.07%, 6.89%), p < 0.00001], and a significant reduction in left ventricular end-diastolic diameter (LVEDD) compared to RVP [MD = -3.98 mm; 95% CI: (-5.88, -2.09 mm), p < 0.0001]. In terms of clinical outcomes, LBBAP was associated with a significantly lower risk of heart failure hospitalizations (HFHs) compared to RVP [OR = 0.26; 95% CI: (0.16, 0.44), p < 0.0001]. However, no significant differences were observed between the two groups in the implant success rate, pacing impedance, or pacing threshold. The RVP group demonstrated a significantly higher R-wave amplitude increase than the LBBAP group [MD = 0.85 mV; 95% CI: (0.23, 1.46), p = .007]. Lastly, there was no significant difference in the incidence of complications between the two groups [OR = 2.12; 95% CI: (0.29, 15.52), p = 0.46].
LBBAP outperforms RVP in several cardiac function indicators, suggesting it may be a superior pacing method for AVB patients with preserved LVEF. However, the small sample size in studies and the result in heterogeneity call for more research to validate these findings and assess LBBAP's long-term effects.
左束支区域起搏(LBBAP)是一种用于房室传导阻滞(AVB)且左心室射血分数(LVEF)保留患者的新技术,与右心室起搏(RVP)相比,可能提供更好的心脏功能。
我们检索数据库和登记处,查找比较LBBAP与RVP在AVB且LVEF保留患者中的研究。我们提取了各种结局的数据,并使用随机效应模型汇总效应估计值。
我们的荟萃分析纳入了14项研究(10项观察性研究和4项随机对照试验),涉及3062例AVB患者。分析显示,与RVP组相比,LBBAP组的QRS波时限显著缩短[MD = -35.56 ms;95%CI:(-39.27,-31.85),p < 0.00001]。LBBAP组患者的左心室射血分数(LVEF)也显著增加[MD = 5.48%;95%CI:(4.07%,6.89%),p < 0.00001],与RVP相比,左心室舒张末期内径(LVEDD)显著减小[MD = -3.98 mm;95%CI:(-5.88,-2.09 mm),p < 0.0001]。在临床结局方面,与RVP相比,LBBAP与心力衰竭住院(HFHs)风险显著降低相关[OR = 0.26;95%CI:(0.16,0.44),p < 0.0001]。然而,两组在植入成功率、起搏阻抗或起搏阈值方面未观察到显著差异。RVP组的R波振幅增加显著高于LBBAP组[MD = 0.85 mV;95%CI:(0.23,1.46),p = 0.007]。最后,两组并发症发生率无显著差异[OR = 2.12;95%CI:(0.29,15.52),p = 0.46]。
在多项心脏功能指标方面,LBBAP优于RVP,这表明它可能是LVEF保留的AVB患者的一种更优起搏方法。然而,研究中的样本量较小以及异质性结果需要更多研究来验证这些发现并评估LBBAP的长期效果。