Department of Cardiology, Zhongshan Hospital of Fudan University, Shanghai Institute of Cardiovascular Diseases, National Clinical Research Center for Interventional Medicine, 180 Fenglin Road, Shanghai 200032, China.
Department of Cardiology, Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University, No. 3 Qingchun East Road, Hangzhou, Zhejiang 310016, China.
Europace. 2022 May 3;24(5):807-816. doi: 10.1093/europace/euab249.
The purpose of our study was to evaluate the feasibility and efficacy of cardiac resynchronization therapy (CRT) via left bundle branch pacing (LBBP-CRT) compared with optimized biventricular pacing (BVP) with adaptive algorithm (BVP-aCRT) in heart failure with reduced left ventricular ejection fraction ≤35% (HFrEF) and left bundle branch block (LBBB).
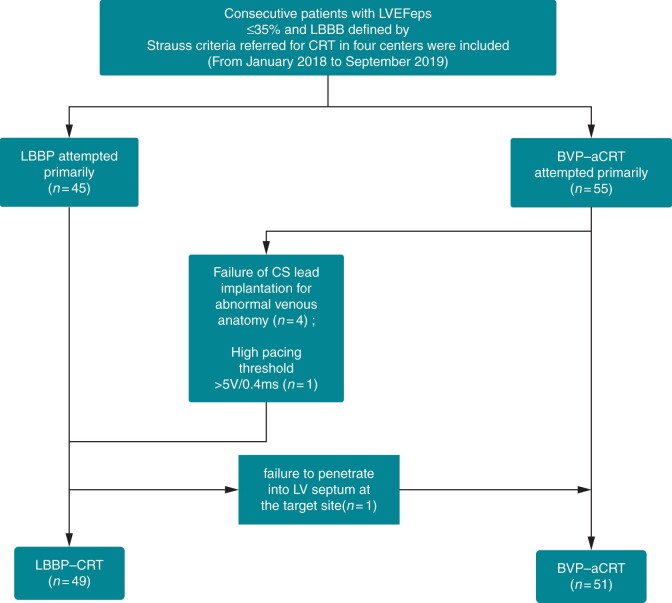
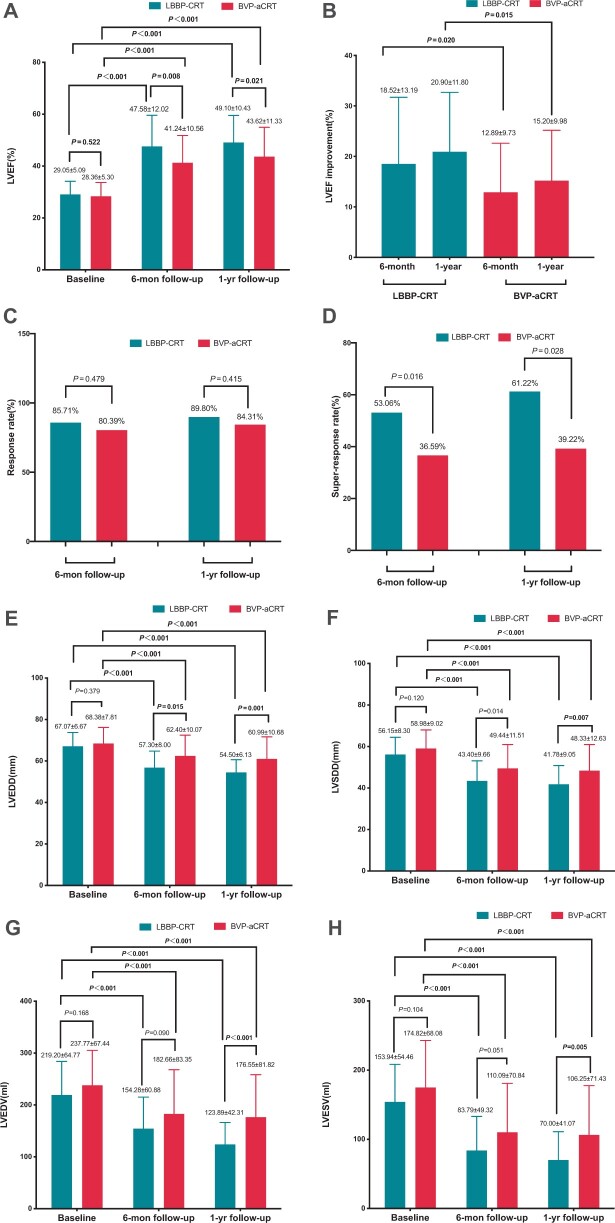
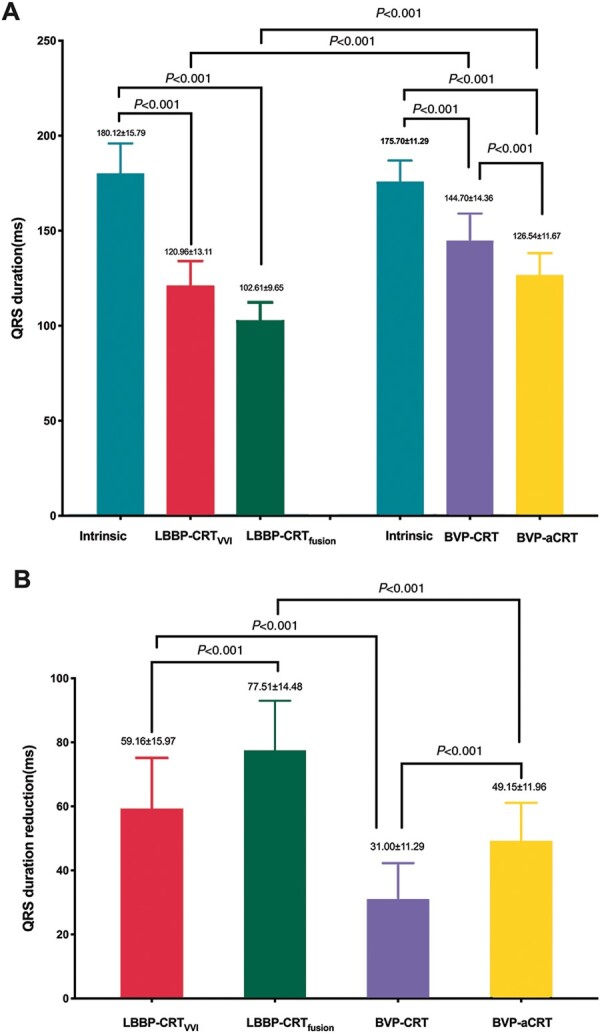
One hundred patients with HFrEF and LBBB undergoing CRT were prospectively enrolled in a non-randomized fashion and divided into two groups (LBBP-CRT, n = 49; BVP-aCRT, n = 51) in four centres. Implant characteristics and echocardiographic parameters were accessed at baseline and during 6-month and 1-year follow-up. The success rate for LBBP-CRT and BVP-aCRT was 98.00% and 91.07%. Fused LBBP had the greatest reduced QRS duration compared to BVP-aCRT (126.54 ± 11.67 vs. 102.61 ± 9.66 ms, P < 0.001). Higher absolute left ventricular ejection fraction (LVEF) and △LVEF was also achieved in LBBP-CRT than BVP-aCRT at 6-month (47.58 ± 12.02% vs. 41.24 ± 10.56%, P = 0.008; 18.52 ± 13.19% vs. 12.89 ± 9.73%, P = 0.020) and 1-year follow-up (49.10 ± 10.43% vs. 43.62 ± 11.33%, P = 0.021; 20.90 ± 11.80% vs. 15.20 ± 9.98%, P = 0.015, P = 0.015). There was no significant difference in response rate between two groups while higher super-response rate was observed in LBBP-CRT as compared to BVP-aCRT at 6 months (53.06% vs. 36.59%, P = 0.016) and 12 months (61.22% vs. 39.22%, P = 0.028) during follow-up. The pacing threshold was lower in LBBP-CRT at implant and during 1-year follow-up (both P < 0.001). Procedure-related complications and adverse clinical outcomes including heart failure hospitalization and mortality were not significantly different in two groups.
The feasibility and efficacy of LBBP-CRT demonstrated better electromechanical resynchronization and higher clinical and echocardiographic response, especially higher super-response than BVP-aCRT in HFrEF with LBBB.
本研究旨在评估左束支区域起搏(LBBP-CRT)与优化的双心室起搏(BVP)与自适应算法(BVP-aCRT)在射血分数降低的心力衰竭(HFrEF)且存在左束支传导阻滞(LBBB)患者中的可行性和疗效。
100 例 HFrEF 且 LBBB 行 CRT 的患者前瞻性地以非随机方式在 4 个中心被纳入,并分为两组(LBBP-CRT,n=49;BVP-aCRT,n=51)。在基线和 6 个月及 1 年随访时,评估植入特征和超声心动图参数。LBBP-CRT 和 BVP-aCRT 的成功率分别为 98.00%和 91.07%。与 BVP-aCRT 相比,融合的 LBBP 使 QRS 时限显著缩短(126.54±11.67 比 102.61±9.66 ms,P<0.001)。在 6 个月(47.58±12.02%比 41.24±10.56%,P=0.008;18.52±13.19%比 12.89±9.73%,P=0.020)和 1 年随访(49.10±10.43%比 43.62±11.33%,P=0.021;20.90±11.80%比 15.20±9.98%,P=0.015)时,LBBP-CRT 也实现了更高的左心室射血分数(LVEF)绝对值和△LVEF。在随访期间,LBBP-CRT 的反应率与 BVP-aCRT 无显著差异,但 LBBP-CRT 的超反应率更高,在 6 个月(53.06%比 36.59%,P=0.016)和 12 个月(61.22%比 39.22%,P=0.028)时更高。与 BVP-aCRT 相比,LBBP-CRT 在植入时和 1 年随访时的起搏阈值更低(均 P<0.001)。两组间手术相关并发症和不良临床结局(包括心力衰竭住院和死亡率)无显著差异。
在 HFrEF 且 LBBB 患者中,LBBP-CRT 的可行性和疗效优于 BVP-aCRT,可实现更好的机电同步,且临床和超声心动图反应更高,尤其是超反应率更高。