Mu Xuemeng, Zhang Hengyan, Zhang Jia
Department of Orthopedic Surgery, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing, China.
Orthop Surg. 2025 Apr;17(4):1067-1074. doi: 10.1111/os.14354. Epub 2025 Jan 9.
Dual energy x-ray absorptiometry (DXA) provides incomplete information about bone strength. There are few data on the relationship between osteoporosis-related examinations and bone strength. The objective of the present study was to determine which osteoporosis-related examinations best predicted trabecular bone strength, and to enhance a formula for predicting bone strength on the basis of bone density examination.
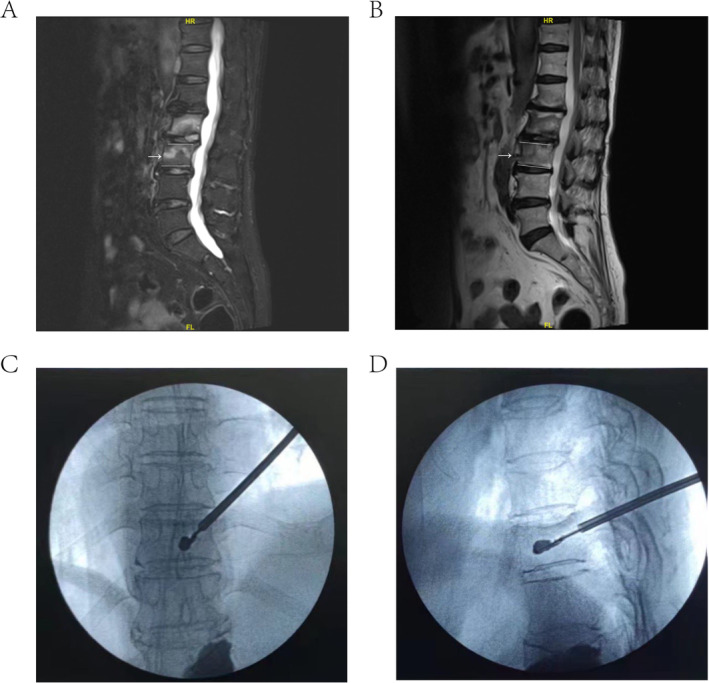
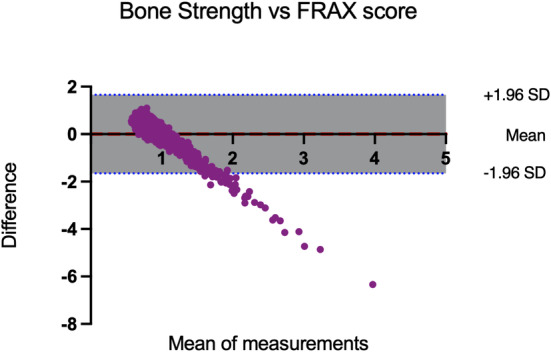
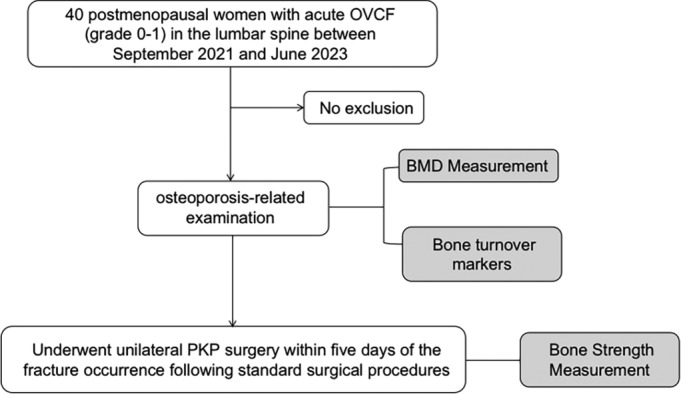
This observational study included postmenopausal women (aged over 50 years) who underwent unilateral percutaneous kyphoplasty (PKP) surgery in the lumbar spine between September 2021 and June 2023. The pressure within each balloon expansion circle was extracted to reflect the true bone strength. The NHANES 2013-2014 data were used to assess the performance of the formula. The performance of the formula was compared with that of the observed actual fractures. Bland-Altman analysis was used to compare the agreement between the formula and the fracture risk assessment tool (FRAX) score.
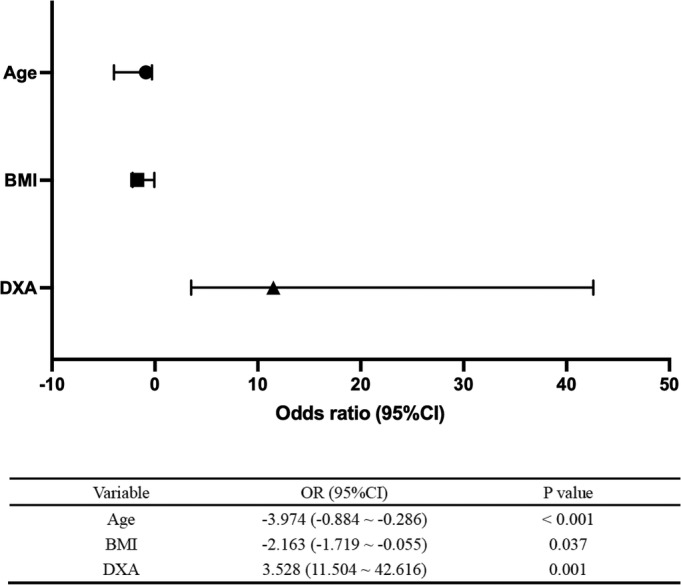
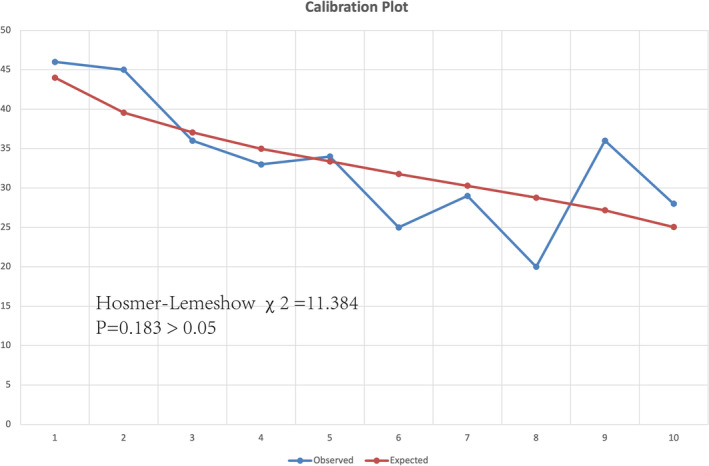
A total of 40 postmenopausal women (mean age ± standard deviation, 70.90 years ± 10.30) were enrolled. The average balloon pressure was 59.23 psi (± 12.40, means ± SDs). The mean BMD of total lumbar spine (average of L1-L4) was 0.89 g/cm ± 0.20 (mean ± standard), and the Pearson correlation coefficient between lumbar BMD and bone strength was 0.516. After adjusting for age and BMI, the DXA response rate to bone strength reached 72%. Calibration plots of the observed actual fractures versus those estimated via the bone strength formula were considered good fits. The Bland-Altman analysis revealed a nonsignificant difference between the formula and the FRAX score in predicting fracture risk.
After adjustment, the DXA response rate to bone strength reached 72%, indicating a strong correlation. In addition, Bone Strength = DXA × 27 - Age × 0.585-BMI × 0.887 + 98.
双能X线吸收法(DXA)提供的骨强度信息不完整。关于骨质疏松症相关检查与骨强度之间关系的数据较少。本研究的目的是确定哪些骨质疏松症相关检查能最佳预测小梁骨强度,并基于骨密度检查改进预测骨强度的公式。
这项观察性研究纳入了2021年9月至2023年6月期间在腰椎接受单侧经皮椎体后凸成形术(PKP)手术的绝经后女性(年龄超过50岁)。提取每个球囊扩张圈的压力以反映真实骨强度。使用2013 - 2014年美国国家健康与营养检查调查(NHANES)数据评估该公式的性能。将该公式的性能与观察到的实际骨折情况进行比较。采用Bland - Altman分析比较该公式与骨折风险评估工具(FRAX)评分之间的一致性。
共纳入40名绝经后女性(平均年龄±标准差,70.90岁±10.30)。球囊平均压力为59.23磅力/平方英寸(±12.40,均值±标准差)。整个腰椎(L1 - L4平均值)的平均骨密度为0.89克/平方厘米±0.20(均值±标准差),腰椎骨密度与骨强度之间的Pearson相关系数为0.516。在调整年龄和体重指数后,DXA对骨强度的反应率达到72%。观察到的实际骨折情况与通过骨强度公式估计的情况的校准图显示拟合良好。Bland - Altman分析显示该公式与FRAX评分在预测骨折风险方面无显著差异。
调整后,DXA对骨强度的反应率达到72%,表明存在强相关性。此外,骨强度 = DXA×27 - 年龄×0.585 - 体重指数×0.887 + 98。