Preeprem Nutnicha, See Emily, Namachivayam Siva P, Gelbart Ben
Pediatric Intensive Care Unit, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Paediatric Intensive Care Unit, Royal Children's Hospital, Melbourne, VIC, Australia.
Crit Care Resusc. 2024 Nov 26;26(4):319-325. doi: 10.1016/j.ccrj.2024.10.001. eCollection 2024 Dec.
Frusemide is a common diuretic administered to critically ill children intravenously, by either continuous infusion (CI) or intermittent bolus (IB). We aim to describe the characteristics of children who receive intravenous frusemide, patterns of use, and incidence of acute kidney injury (AKI), and to investigate factors associated with commencing CI.
Retrospective observational study.
Paediatric intensive care unit (PICU), the Royal Children's Hospital Melbourne.
Children who received intravenous frusemide during PICU admission lasting ≥24 h between 2017 and 2022.
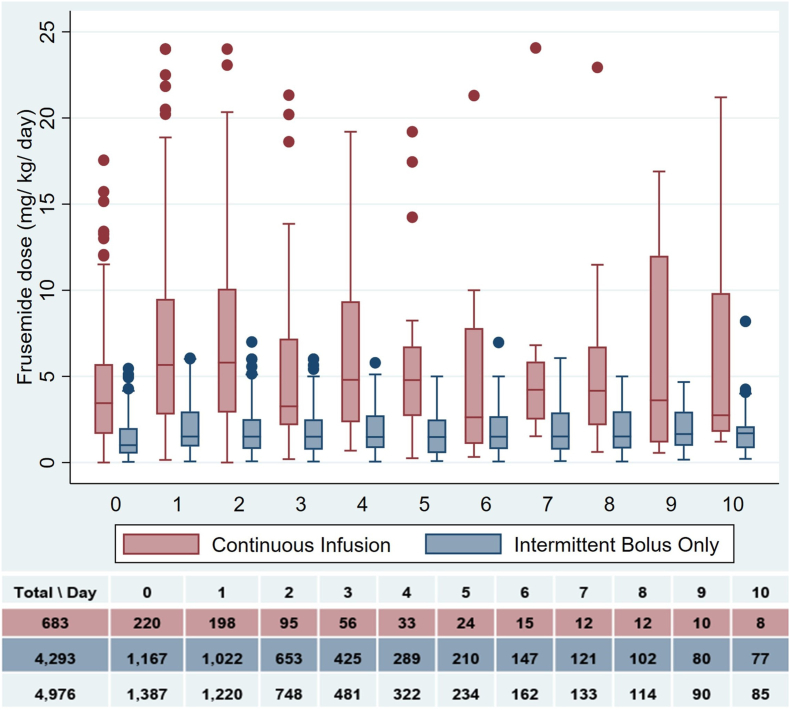
The primary outcome was the daily dose of frusemide. Secondary outcomes included timing of therapy from PICU admission, fluid balance at frusemide initiation, additional diuretic therapy, and the incidence of AKI at admission and frusemide initiation. Children who received CI were compared with those who received IB only using multivariable logistic regression analyses.
Nine thousand three ninety-four children were admitted during the study period. A total of 1387 children (15 %) received intravenous frusemide, including 220 children (16 %) by CI. The CI group were younger (132 vs 202 days, = 0.01), had higher PIM-3 scores (2.2 vs 1.5, -value <0.001), more congenital heart disease (CHD) (72.3 % vs 60.6 %, <0.01), and higher incidence and severity of AKI at frusemide initiation than the IB group (65.7 % vs 40.1 %, -value <0.001). CI were commenced later than IB (46 vs 19 h into admission, <0.001) and at higher doses (4.3 vs 1.5 mg/kg/day, -value <0.001). In multivariable analyses, CHD (aOR 1.67, 95 % CI 1.16-2.40, <0.01) was associated with CI.
Frusemide infusions are administered more commonly to children with CHD, later in PICU admission, and at higher daily doses compared to IB. Children who receive CI have a higher incidence and severity of AKI at initiation.
呋塞米是一种常用于危重症儿童的利尿剂,通过持续输注(CI)或间歇推注(IB)静脉给药。我们旨在描述接受静脉注射呋塞米的儿童的特征、使用模式和急性肾损伤(AKI)的发生率,并调查与开始CI相关的因素。
回顾性观察研究。
墨尔本皇家儿童医院儿科重症监护病房(PICU)。
2017年至2022年期间在PICU住院持续≥24小时并接受静脉注射呋塞米的儿童。
主要结局是呋塞米的每日剂量。次要结局包括从PICU入院开始治疗的时间、开始使用呋塞米时的液体平衡、额外的利尿治疗,以及入院时和开始使用呋塞米时AKI的发生率。仅使用多变量逻辑回归分析将接受CI的儿童与接受IB的儿童进行比较。
在研究期间,共有9394名儿童入院。共有1387名儿童(15%)接受了静脉注射呋塞米,其中220名儿童(16%)通过CI给药。CI组儿童年龄更小(132天对202天,P = 0.01),PIM-3评分更高(2.2对1.5,P值<0.001),先天性心脏病(CHD)更多(72.3%对60.6%,P<0.01),开始使用呋塞米时AKI的发生率和严重程度高于IB组(65.7%对40.1%,P值<0.001)。CI开始的时间比IB晚(入院后46小时对19小时,P<0.001),且剂量更高(4.3对1.5mg/kg/天,P值<0.001)。在多变量分析中,CHD(调整后比值比1.67,95%可信区间1.16 - 2.40,P<0.01)与CI相关。
与IB相比,CHD儿童更常接受呋塞米输注,在PICU入院后期进行,且每日剂量更高。接受CI的儿童在开始使用时AKI的发生率和严重程度更高。