Grega Tomas, Kmochova Klara, Hejcmanova Katerina, Ngo Ondrej, Brodyuk Nadija, Majek Ondrej, Bures Jan, Urbanek Petr, Zavoral Miroslav, Suchanek Stepan
Department of Internal Medicine, 1st Faculty of Medicine Charles University, Military University Hospital, Prague, Czechia.
Department of Gastrointestinal Oncology, Military University Hospital, Prague, Czechia.
Sci Rep. 2025 Jan 9;15(1):1414. doi: 10.1038/s41598-025-85669-w.
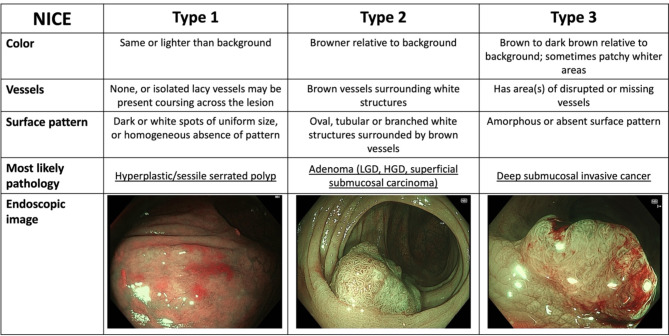
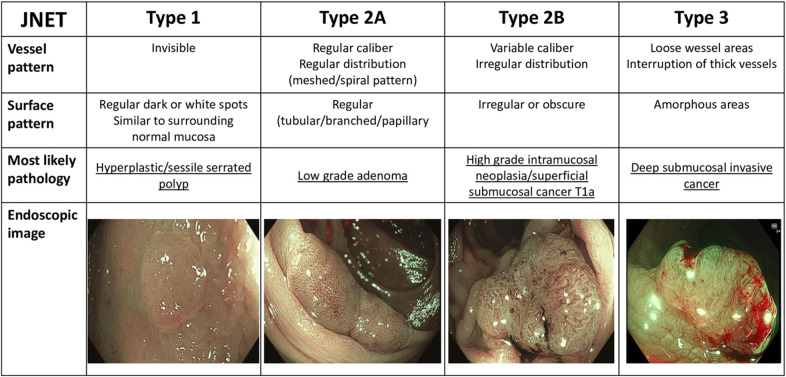
We assessed the diagnostic performance of the Narrow-Band Imaging (NBI) International Colorectal Endoscopic Classification (NICE) and the Japan NBI Expert Team classification (JNET) in predicting histological outcomes of advanced colorectal lesions. Additionally, we evaluated the sensitivity and positive predictive value (PPV) of the JNET and NICE classifications individually for high-grade lesions (including HGD adenomas, intramucosal carcinomas, and T1 carcinomas). This was a retrospective analysis of prospectively collected data, involving 211 patients (130 men, mean age 60 years) who underwent colonoscopy with endoscopic resection of advanced colorectal neoplasia (lesions ≥ 10 mm). Lesions were classified using both NICE and JNET criteria, and final histopathological results were used for comparison. Of the 257 lesions analyzed, the NICE classification accurately classifies a large proportion of lesions (93.8%). In JNET classification we observed 77.4% correctly classified lesions. Specifically, the sensitivity and positive predictive value (PPV) of the NICE classification for high-grade lesions were 100% and 24.4%, respectively. For the JNET classification, the sensitivity and PPV for high-grade lesions were 56.6% and 57.7%, respectively. The JNET classification, with a positive predictive value of 57.7% for high-grade colorectal lesions (including HGD adenomas, intramucosal carcinomas, and T1 carcinomas), should be used for decision-making regarding appropriate subsequent endoscopic therapy.
我们评估了窄带成像(NBI)国际结直肠内镜分类(NICE)和日本NBI专家团队分类(JNET)在预测晚期结直肠病变组织学结果方面的诊断性能。此外,我们分别评估了JNET和NICE分类对高级别病变(包括高级别上皮内瘤变腺瘤、黏膜内癌和T1期癌)的敏感性和阳性预测值(PPV)。这是一项对前瞻性收集数据的回顾性分析,涉及211例患者(130名男性,平均年龄60岁),他们接受了结肠镜检查并对晚期结直肠肿瘤(病变≥10毫米)进行了内镜切除。使用NICE和JNET标准对病变进行分类,并将最终组织病理学结果用于比较。在分析的257个病变中,NICE分类准确分类了很大一部分病变(93.8%)。在JNET分类中,我们观察到77.4%的病变分类正确。具体而言,NICE分类对高级别病变的敏感性和阳性预测值分别为100%和24.4%。对于JNET分类,高级别病变的敏感性和PPV分别为56.6%和57.7%。JNET分类对高级别结直肠病变(包括高级别上皮内瘤变腺瘤、黏膜内癌和T1期癌)的阳性预测值为57.7%,应用于有关后续适当内镜治疗的决策。