Schattner Ami, Rokach Ariel, Vernea Fiona, Spector Maria, Filanovsky Kalman
The Faculty of Medicine, Hebrew University and Hadassah Medical School, Jerusalem, Israel.
Departments of Pulmonology (AR), Pathology (FV) and Imaging (MS), Shaare Zedek Medical Center, Jerusalem, Israel.
Eur J Case Rep Intern Med. 2024 Dec 17;11(12):004997. doi: 10.12890/2024_004997. eCollection 2024.
There is little information in the literature on the early, sub-clinical stage and laboratory test results in patients with primary mucosa-associated lymphoid tissue (MALT) lymphoma of the lung, a rare disease.
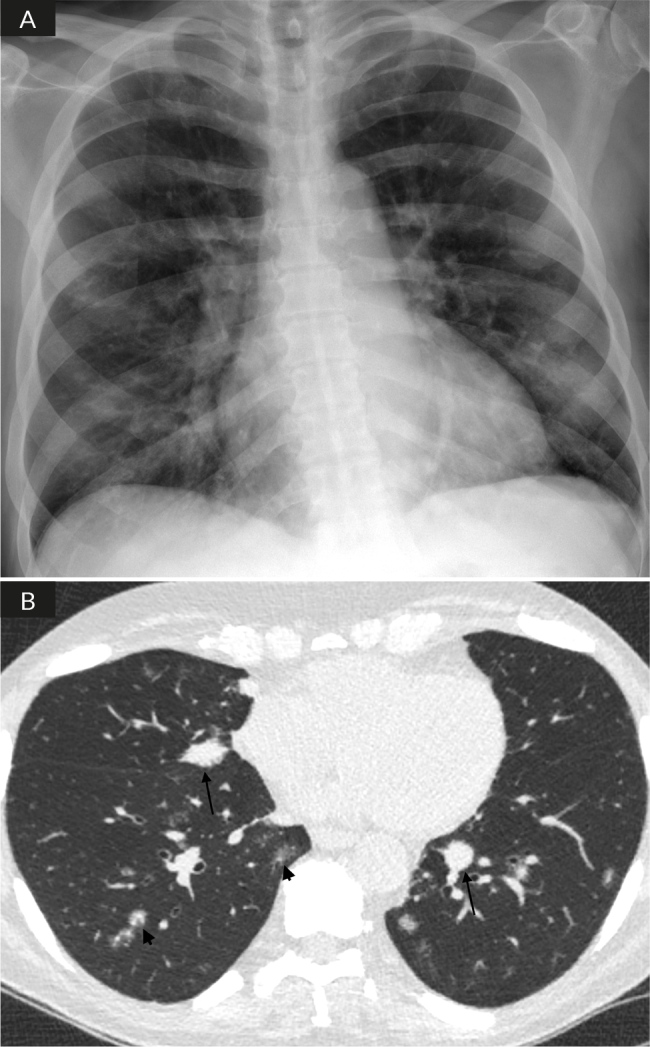
In a 75-year-old man, an open lung biopsy-confirmed diagnosis of primary pulmonary lymphoma was preceded by almost six months of anaemia of inflammatory disease and monocytosis without any pulmonary symptoms. When he developed a dry cough, increasing dyspnoea and marked weight loss, these changes deepened and became associated with reactive thrombocytosis; markedly increased ferritin and C-reactive protein (positive acute-phase reactants), as well as reduced albumin and transferrin (negative acute-phase reactants). Globulins increased, due to an increase in the alpha1, alpha2 and gamma fractions, and mild hyponatraemia developed due to the syndrome of inappropriate antidiuretic hormone secretion (SIADH) secondary to the intrathoracic disease. All these changes were completely reversible following successful treatment and complete remission.
The previously unreported detailed laboratory features of early, sub-clinical and advanced primary pulmonary lymphoma are presented. When a potentially susceptible patient develops an unexplained anaemia of inflammatory disease, primary pulmonary lymphoma should be added to the differential diagnosis.
B-cell pulmonary lymphoma without extra-pulmonary disease (primary pulmonary lymphoma) remains a rare entity, often arising from mucosa-associated lymphoid tissue, presenting with non-specific symptoms (cough, dyspnoea) and imaging (nodules <5 cm or areas of consolidation on CT), and diagnosed by an adequate biopsy.Our patient's course demonstrates early, pre-clinical changes: anaemia of inflammation and monocytosis, which became more severe as symptoms developed and imaging abnormalities progressed, and was associated with marked acute-phase response (for example, substantially increased ferritin levels), increased globulins and hyponatraemia due to the syndrome of inappropriate antidiuretic hormone secretion.In patients with unexplained anaemia of inflammatory disease, occult pulmonary lymphoma should be considered in the differential diagnosis.
原发性肺黏膜相关淋巴组织(MALT)淋巴瘤是一种罕见疾病,关于其早期亚临床阶段及实验室检查结果的文献资料较少。
一名75岁男性,在经开放性肺活检确诊为原发性肺淋巴瘤之前,已有近6个月的炎症性贫血和单核细胞增多症,且无任何肺部症状。当他出现干咳、进行性呼吸困难和明显体重减轻时,这些变化加剧,并伴有反应性血小板增多症;铁蛋白和C反应蛋白(急性期反应物阳性)显著升高,白蛋白和转铁蛋白(急性期反应物阴性)降低。球蛋白增加,这是由于α1、α2和γ组分增加所致,并且由于胸腔内疾病继发抗利尿激素分泌不当综合征(SIADH)而出现轻度低钠血症。所有这些变化在成功治疗并完全缓解后均可完全逆转。
本文呈现了此前未报道的原发性肺淋巴瘤早期、亚临床期及进展期的详细实验室特征。当潜在易感患者出现不明原因的炎症性贫血时,应将原发性肺淋巴瘤纳入鉴别诊断。
无肺外疾病的B细胞性肺淋巴瘤(原发性肺淋巴瘤)仍然是一种罕见疾病,通常起源于黏膜相关淋巴组织,表现为非特异性症状(咳嗽、呼吸困难)和影像学表现(CT上<5 cm的结节或实变区域),并通过充分的活检进行诊断。我们患者的病程显示出早期的临床前变化:炎症性贫血和单核细胞增多症,随着症状发展和影像学异常进展而加重,并与明显的急性期反应(例如铁蛋白水平大幅升高)、球蛋白增加以及抗利尿激素分泌不当综合征导致低钠血症有关。对于不明原因炎症性贫血的患者,鉴别诊断时应考虑隐匿性肺淋巴瘤。