Salati Michele, Andolfi Marco, Roncon Alberto, Guiducci Gian Marco, Xiumè Francesco, Tiberi Michela, Nanto Anna Chiara, Cingolani Sara, Ricci Eleonora, Refai Majed
Unit of Thoracic Surgery, AOU of Marche, 60126 Ancona, Italy.
Unit of Rehabilitation Medicine, AOU of Marche, 60126 Ancona, Italy.
Cancers (Basel). 2024 Dec 26;17(1):32. doi: 10.3390/cancers17010032.
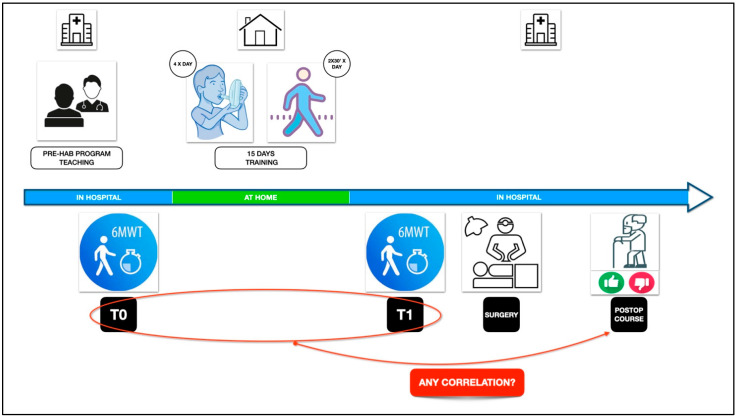
The purpose of the present study was to verify if performance in the 6-min walking test (6MWT) during the preoperative evaluation phase is associated with the development of cardiopulmonary postoperative complications in patients who underwent uniportal VATS (U-VATS) for lung cancer.
This retrospective, monocentric study included patients submitted to U-VATS anatomical lung resections (March 2022-December 2023). The patients were enrolled in a preoperative rehabilitation program carried out 15 days before surgery. The 6MWT was performed at counseling (T0) and after pre-habilitation (T1). Univariate analysis followed by logistic regression verified the association of baseline patients' characteristics and performance in the 6MWT (meters walked during T0 and T1 and the difference between T1 and T0-T1-T0 variation) with postoperative cardiopulmonary complications (CPCs). Youde's index was used to establish the optimal cut-offs for ergometric parameters significantly correlated with CPCs.
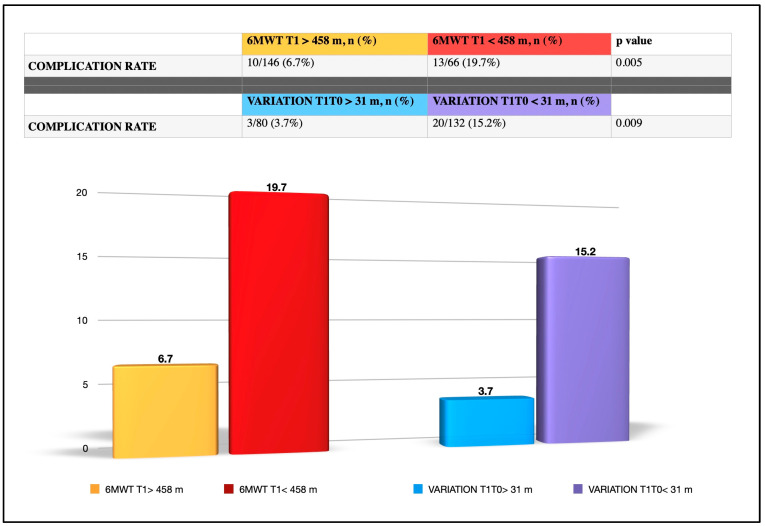
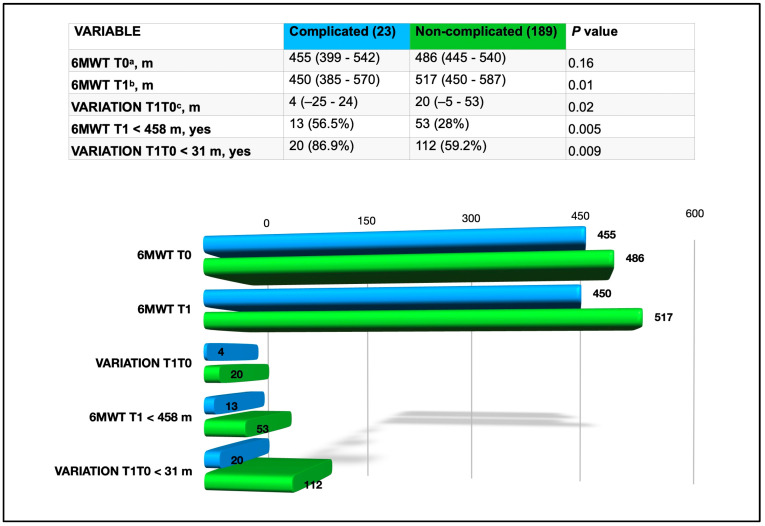
We enrolled 212 patients scheduled to undergo U-VATS lung resection (lobectomies: 177; bilobectomies: 2; segmentectomies: 33). Twenty-three (10.8%) patients developed CPCs. None of the baseline patients' characteristics were associated with CPCs. Complicated patients showed more significant differences compared to non-complicated ones for meters walked during the 6MWT T1 (6MWT-T1-complicated: 450 vs. 6MWT-T1-non-complicated: 517; : 0.01) and for variation-T1-T0 (variation-T1-T0-complicated: 4 m vs. variation-T1-T0-non-complicated: 20 m; : 0.02). The best cut-offs for discriminating between patients with CPCs and those with uneventful courses were 458 m for 6MWT-T1 and 31 m for variation-T1-T0. After multivariate analysis, 6MWT-T1 < 458 m and variation-T1-T0 < 31 m were the unique parameters independently correlated with CPCs (: 0.03 and : 0.05, respectively).
The 6MWT results (in particular, 6MWT-T1 < 458 m and variation-T1-T0 < 31 m) in the context of a pre-habilitation program are associated with the development of CPCs after U-VATS lung resection.
本研究旨在验证术前评估阶段6分钟步行试验(6MWT)的表现是否与接受单孔电视辅助胸腔镜手术(U-VATS)治疗肺癌患者的术后心肺并发症的发生有关。
这项回顾性单中心研究纳入了接受U-VATS解剖性肺切除术的患者(2022年3月至2023年12月)。患者参加了术前15天进行的康复计划。在咨询时(T0)和康复前(T1)进行6MWT。单因素分析后进行逻辑回归,以验证患者基线特征和6MWT表现(T0和T1期间行走的米数以及T1与T0之间的差异 - T1 - T0变化)与术后心肺并发症(CPC)之间的关联。使用尤德指数确定与CPC显著相关的运动参数的最佳临界值。
我们纳入了212例计划接受U-VATS肺切除术的患者(肺叶切除术:177例;双叶切除术:2例;肺段切除术:33例)。23例(10.8%)患者发生了CPC。患者的基线特征均与CPC无关。与未发生并发症的患者相比,发生并发症的患者在6MWT T1期间行走的米数(6MWT - T1 - 发生并发症者:450米 vs. 6MWT - T1 - 未发生并发症者:517米;:0.01)以及T1 - T0变化(T1 - T0变化 - 发生并发症者:4米 vs. T1 - T0变化 - 未发生并发症者:20米;:0.02)方面表现出更显著的差异。区分发生CPC的患者和病程平稳的患者的最佳临界值为6MWT - T1为458米,T1 - T0变化为31米。多因素分析后,6MWT - T1 < 458米和T1 - T0变化 < 31米是与CPC独立相关的唯一参数(分别为:0.03和:0.05)。
在康复前计划的背景下,6MWT结果(特别是6MWT - T1 < 458米和T1 - T0变化 < 31米)与U-VATS肺切除术后CPC的发生有关。