Romano Giulio, Fiorini Nicholas, Bertoni Martina, Rondinella Stefania, Di Pietra Laura, Cola Marco F, De Martin Paolo, Tonizzo Maurizio, Desinan Lorenzo, Boari Benedetta, Manfredini Roberto, Colussi GianLuca
Nephrology Unit, Department of Medicine, University of Udine, 33100 Udine, Italy.
Hypertension and Ultrasound Vascular Unit, Division of Internal Medicine, "Santa Maria degli Angeli" City Hospital of Pordenone, Azienda Sanitaria Friuli Occidentale, 33170 Pordenone, Italy.
J Clin Med. 2025 Jan 3;14(1):228. doi: 10.3390/jcm14010228.
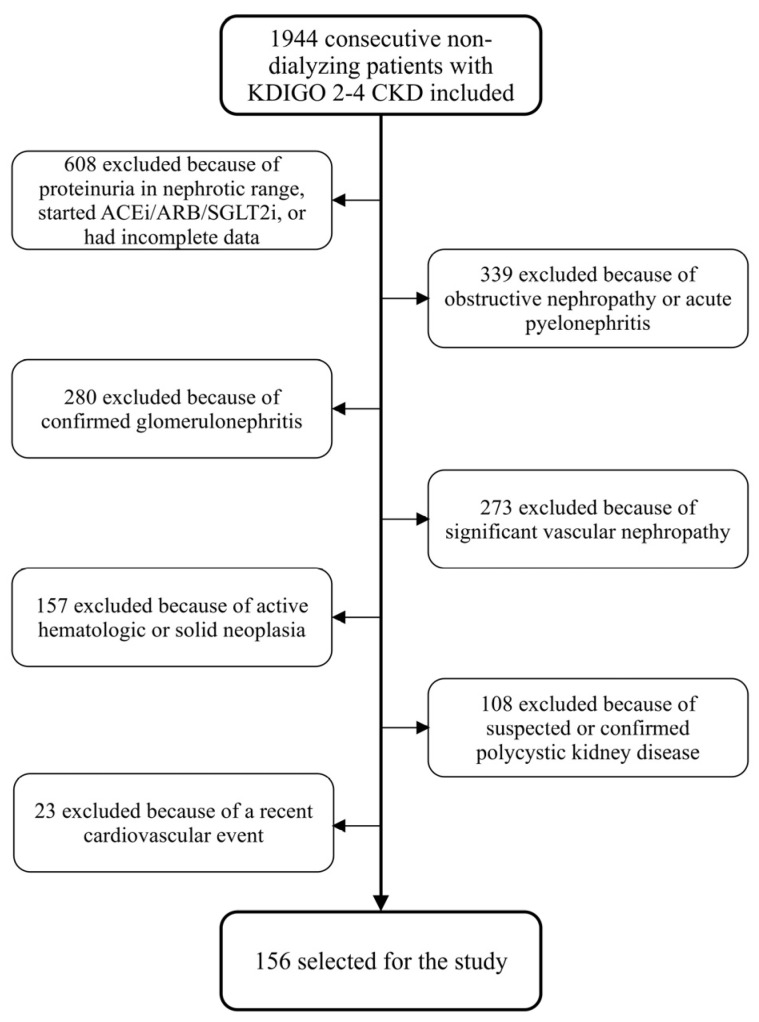
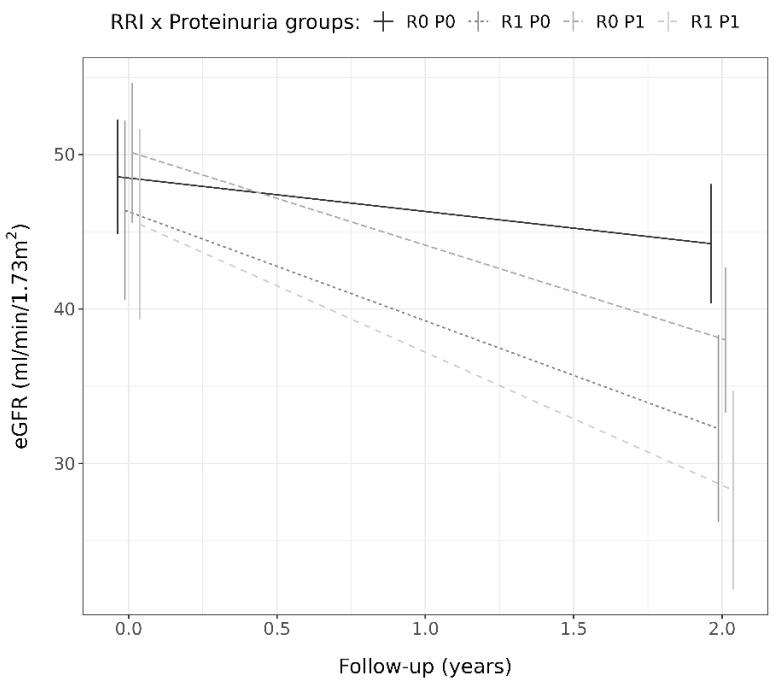
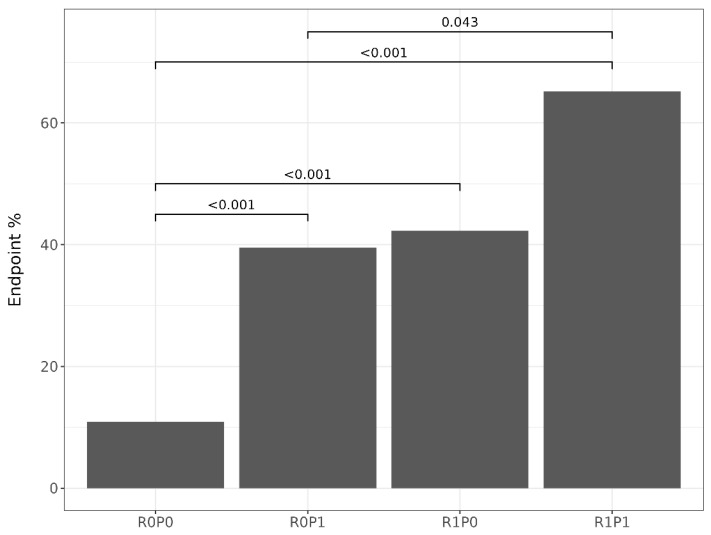
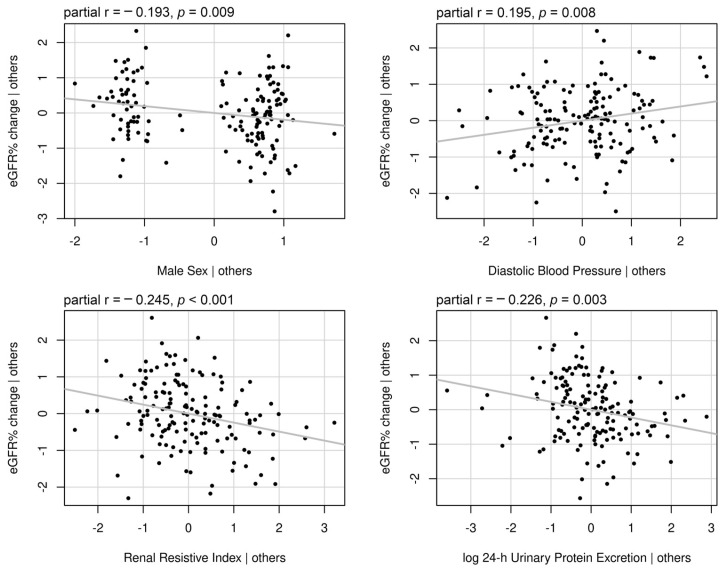
An increased renal resistive index (RRI) and proteinuria can predict an estimated glomerular filtration rate (eGFR) decline in patients with chronic kidney disease (CKD) of various causes. This study hypothesized that the RRI and proteinuria interact to determine disease progression in patients with CKDs of unknown origin. : One hundred and fifty six patients (age 76.0 ± 8.1 years, 63.5% males) were analyzed for anthropometric, kidney morphology, blood pressure, 24 h urinary protein excretion, and RRI. The CKD-EPI equation was used to calculate the eGFR at baseline and after a two-year follow-up. Patients with an elevated (≥0.80) or normal (<0.80) RRI and significant (≥150 mg/day) or physiological (<150 mg/day) proteinuria were evaluated for the likelihood of at least a 30% drop in the eGFR or the onset of end-stage kidney disease (endpoint). : Hypertension and diabetes were the predominant cardiovascular risk factors (90.4%). Fifty patients (32%) met the endpoint. Elevated RRIs (odds ratio, OR, 4.28; 95% confidence interval, CI, 1.82-10.6; = 0.001) and significant proteinuria (OR 3.59, 95% CI 1.59-8.48, = 0.003) were independent predictors of the endpoint in a multivariate logistic model. Patients with an elevated RRI and significant proteinuria were more likely to meet the endpoint (R1P1: 65.2%) compared to those with only proteinuria (R0P1: 39.5%, = 0.043) or both normal factors (R0P0: 10.9%, < 0.001) but not to those with only an elevated RRI (R1P0: 42.3%, = 0.094). Continuous RRIs (partial correlation r = -0.245, < 0.001) and 24 h urinary protein excretion (partial r = -0.226, = 0.003) were inversely and independently correlated with eGFR% change. R1P1 showed a higher eGFR% reduction (-38.0% ± 20.4%) compared to R0P1 (-25.3% ± 19.0%, = 0.043) and R0P0 (-8.8% ± 25.1%, < 0.001) but not to R1P0 (-29.6% ± 21.0%, = 0.192). : An increased RRI and proteinuria were independent predictors of disease progression. When interaction was considered, the negative effect of an elevated RRI on CKD progression was evident in both proteinuric and non-proteinuric patients, whereas the negative effect of proteinuria on disease progression was only significant in patients with no elevated RRIs.
肾阻力指数(RRI)升高和蛋白尿可预测各种病因的慢性肾脏病(CKD)患者的估计肾小球滤过率(eGFR)下降。本研究假设,RRI和蛋白尿相互作用,决定不明原因CKD患者的疾病进展。对156例患者(年龄76.0±8.1岁,63.5%为男性)进行人体测量、肾脏形态、血压、24小时尿蛋白排泄和RRI分析。采用CKD-EPI方程计算基线和两年随访后的eGFR。对RRI升高(≥0.80)或正常(<0.80)以及蛋白尿显著(≥150mg/天)或生理性(<150mg/天)的患者,评估其eGFR至少下降30%或终末期肾病发生(终点)的可能性。高血压和糖尿病是主要的心血管危险因素(90.4%)。50例患者(32%)达到终点。在多因素逻辑模型中,RRI升高(比值比,OR:4.28;95%置信区间,CI:1.82-10.6;P=0.001)和显著蛋白尿(OR 3.59,95%CI 1.59-8.48,P=0.003)是终点的独立预测因素。与仅蛋白尿患者(R0P1:39.5%,P=0.043)或两个因素均正常患者(R0P0:10.9%,P<0.001)相比,RRI升高且蛋白尿显著的患者更易达到终点(R1P1:65.2%),但与仅RRI升高患者(R1P0:42.3%,P=0.094)相比无差异。连续RRI(偏相关r=-0.245,P<0.001)和24小时尿蛋白排泄(偏r=-0.226,P=0.003)与eGFR%变化呈负向独立相关。与R0P1(-25.3%±19.0%,P=0.043)和R0P0(-8.8%±25.1%,P<0.001)相比,R1P1的eGFR%降低幅度更大(-38.0%±20.4%)。但与R1P0(-29.6%±21.0%,P=0.192)相比无差异。RRI升高和蛋白尿是疾病进展的独立预测因素。当考虑相互作用时,RRI升高对CKD进展的负面影响在蛋白尿和无蛋白尿患者中均明显,而蛋白尿对疾病进展的负面影响仅在RRI未升高的患者中显著。